Transcription of The South Korean Health Care System - MED
1 206 JMAJ, May / June 2009 Vol. 52, No. 3 International Medical CommunityThe South Korean Health care SystemJMAJ 52(3): 206 209, 2009 Young Joo SONG*1in medical services. Most private medical facili-ties are located in urban areas, and around 90%of physicians are concentrated in cities while80% of the population lives in urban Delivery System : Koreanpatients have freedom of choice1 Korean patients can go to any doctor or anymedical institution, including hospitals, whichthey choose. The referral arrangement System isdivided into two steps.
2 The patient can go to anymedical practitioner office except specializedgeneral hospitals. If the patient wants to go to asecondary hospital, he/she has to present a referralslip issued by the medical practitioner who diag-nosed him/her first. There are some exceptions:in the case of childbirth, emergency medical care ,dental care , rehabilitation, family medicine ser-vices, and hemophiliac disease, the patient can goto any hospital without a referral Arms of healthcare SecuritySouth Korea s healthcare security System has threearms: the National Health Insurance Program,Medical Aid Program, and Long-term care Insur-ance Health Insurance Program3 History.
3 Universal coverage for all citizensThe first Health insurance law in South Korea,the Medical Insurance Act, came into force inDecember 1963. From July 1977, all companieswith more than 500 employees were required toprovide a Health insurance program and separatehealth insurance societies were established. InJanuary 1979, the insurance coverage require-ment was expanded to companies with more than*1 Takemi Fellow, Department of Global Health and Population, Harvard School of Public Health , Boston, MA, USA Director of Policy & public relations, Ministry of Health , Welfare and Family Affairs (MIHWAF).
4 Background: Improvement of livingquality1 The quality of Korean people s lives has beenincreasingly improved in general due to the devel-opment of medical technology. The average lifeexpectancy for males increased from in the1960s to in 2006. The change in average lifeexpectancy for females is even more startling,from in the 1960s to in 2006. In 2007, thecrude birth rate was and the crude death Infant mortality is also decreasing gradually,from per 1,000 live births in the 1960s to 1,000 in 2005.
5 The total fertility rate is sharplydecreasing, from in 1985 to in , the increasing elderly populationand decreasing birth rate are changing familystructure in South Korea. The aging population isalso becoming a social burden due to increasingmedical Personnel: Over 91,000physicians1In South Korea, only authorized healthcare pro-fessionals can provide Health services. The MedicalLaw stipulates that only doctors, dentists, nurses,oriental medical doctors, and midwives licensedby the Ministry of Health , Welfare and FamilyAffairs (MIHWAF)
6 Can provide Health s aides, acupuncturists, and massage thera-pists are described as quasi-medical of 2007, there were 91,400 physicians, 23,114dentists, 16,663 oriental medical doctors, 57,176pharmacists, 8,587 midwives, and 235, 687 nursesin South major problem concerning healthcareresources in South Korea is regional disparities207 JMAJ, May / June 2009 Vol. 52, No. 3300 employees, public servants, and private schoolemployees. In January 1988, self-employed peoplein rural areas were included under this year 1989 is the most important year inthe history of South Korean National HealthInsurance Program.
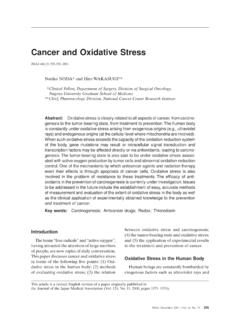
7 In July, the Health insuranceprogram for urban areas was expanded to includethe self-employed. It took 12 years from the estab-ishment of the Medical Insurance Act to achieveuniversal Health insurance coverage for all citi-zens. About ten years later, in 2000, all healthinsurance societies were integrated into a singleinsurer, the National Health Insurance and operationThe National Health Insurance Program isbroadly divided into four parts (Fig. 1). Firstly,the MIHWAF is in charge of supervision andpolicy decisions.
8 It supervises the operation ofthe National Health Insurance Program throughthe formulation and implementation of , the National Health InsuranceCorporation (NHIC) is in charge of managingNational Health Insurance Program, namely theenrollment of insured people and their depen-dents, collection of contributions, and setting ofmedical fee , the Health Insurance Review Agency(HIRA) is in charge of reviewing medical feesand Health care evaluation. After receiving medi-cal care , the patient can submit a claim to HIRA requesting a review of his/her medical fees, andthe NHIC may reimburse the , medical care institutions providehealthcare services.
9 They are directed and super-vised by the coverage and payment ofcontribution4,5 All people in South Korea are eligible for cover-age under the National Health Insurance Program(Table 1). In 2006, the total number of coveredpeople was over 47 million, or over of thetotal population. The insured are divided intotwo groups: employee insured and self-employedinsured. The employee insured category includesTheInsuredNHIC management ofhealth insurancemedical fees reviews, Health care evaluationcontributionsnotification ofreview resultssubmitting medicalfees claimsreimbursementprovidinghealth caredirection andsupervisiondirection andsupervisiondirection andsupervisionMedical CareInstitutionsHIRAM inistry ofHealthand Welfare(Source: Health Insurance Review & Assessment Service)Fig.
10 1 The structure of the National Health Insurance ProgramTHE South Korean Health care SYSTEM208 JMAJ, May / June 2009 Vol. 52, No. 3the insured person s spouse, descendants, brothersor sisters, and direct lineal ascendants. Insuredemployees pay of their average salary incontribution payments. Contribution rates changeevery self-employed insured category includespeople excluded from the category of insuredemployee. Their contribution amount is set tak-ing into account their income, property, livingstandard, and rate of participation in economicactivities.