Transcription of Use of Cholecystostomy Tubes in the Management …
1 Use of Cholecystostomy Tubes in the Managementof patients with Primary Diagnosis ofAcute CholecystitisNicole Cherng,BS, Elan T Witkowski,MD, Erica B Sneider,MD, Jason T Wiseman,MD,Joanne Lewis,NP, Demetrius EM Litwin,MD,MBA,FACS, Heena P Santry,MD,MPH,Mitchell Cahan,MD,FACS, Shimul A Shah,MD,FACSBACKGROUND: Management of patients with severe acute cholecystitis (AC) remains controversial. In settingswhere laparoscopic cholecystectomy (LC) can be technically challenging or medical risks areexceedingly high, surgeons can choose between different options, including LC conversion toopen cholecystectomy or surgical Cholecystostomy tube (CCT) placement, or initial percuta-neous CCT. We reviewed our experience treating complicated AC with CCT at a tertiary-careacademic medical DESIGN:All adult patients (n 185) admitted with a primary diagnosis of AC and who received CCTfrom 2002 to 2010 were identified retrospectively through billing and diagnosis :Mean patient age was 71 years and 80% had 1 comorbidity (mean ).
2 Seventy-eight percentof CCTs were percutaneous CCT placement and 22% were surgical CCT placement. Medianlength of stay from CCT insertion to discharge was 4 days. The majority (57%) of patientseventually underwent cholecystectomy performed by 20 different surgeons in a median of 63days post-CCT (range 3 to 1,055 days); of these, 86% underwent LC and 13% underwent openconversion or open cholecystectomy. In the radiology and surgical group, 50% and 80%underwent subsequent cholecystectomy, respectively, at a median of 63 and 60 days surgical or percutaneous CCT placement, approximately the same proportion ofpatients (85% to 86%) underwent LC as definitive :This 9-year experience shows that use of CCT in complicated AC can be a desirablealternative to open cholecystectomy that allows most patients to subsequently undergo studies are underway to determine the differences in cost, training paradigms,and quality of life in this increasingly high-risk surgical population.
3 (J Am Coll Surg 2012;214:196 201. 2012 by the American College of Surgeons)Acute cholecystitis (AC) often arises from gallstone disease, acondition that annually affects 20 million individuals in theUnited addition, acute calculous cholecystitis isassociated with increased overall, cardiovascular disease, andcancer acute acalculous cholecystitis isless common, it is frequently observed in critically ill and el-derly patients , and is associated with a high incidence of gan-grene and standard treatment for AC is laparo-scopic cholecystectomy (LC), yet Management of critically illand complex patients with AC remains options include open cholecystectomy (OC), conver-sion to open (CONV) procedure, or placement of a cholecys-tostomy tube surgically (sCCT). For elderly patients oryounger patients with substantial comorbidities, the risk ofgeneral anesthesia might be greater than the proven benefits ofoperative less invasive radiologic procedure,percutaneous Cholecystostomy tube placement (pCCT) fol-lowed by interval cholecystectomy, is another option for thesehigh-risk patients .
4 CCT allows for adequate and immediatedecompression and drainage of an acutely inflamed gallblad-der, and can be used as a definitive treatment or a transientmeasure for decreasing inflammation or recovery from criticalillness. There is still debate about how long a tube shouldremain in a patient and whether subsequent cholecystectomyis Information: Authors have nothing to disclose. Timothy JEberlein, Editor-in-Chief, has nothing to October 12, 2011; Revised November 8, 2011; Accepted November10, the Department of Surgery, Surgical Outcomes Analysis & Research(SOAR), University of Massachusetts Medical School, Worcester, address: Shimul A Shah, MD, FACS, Department of Sur-gery, University of Massachusetts Medical School, 55 Lake Ave North, S6-432, Worcester, MA 01655. 2012 by the American College of SurgeonsISSN 1072-7515/12/$ by Elsevier studies describing trends of AC patients treatedwith CCT have either been small scale in patient popula-tion or examined percutaneous CCT placement only andnot surgically placed addition, most studies in-vestigating the use of CCTs have been in critically ill pa-tients who were not admitted with AC or presented withAC as their primary diagnosis.
5 The purpose of this reportwas to determine the role of CCTs in the Management ofAC. We aimed to review our experience with both sCCTsand pCCTs used to treat patients with AC at a tertiary carecenter and determine whether there was a benefit to thesepatients compared with conventional therapy of open con-version or and study populationA database was created containing all patients who wereadmitted at UMass Memorial Center with a primary diag-nosis of AC as described by our group cohort, all patients who received a CCT, either sCCTor pCCT, during their hospital stay from January 1, 2002to January 1, 2011, were identified (n 185). Acute com-plicated cholecystitis was defined as the presence of AC inpatients with medical comorbidities that would deem themhigh risk for University of Massachu-setts Institutional Review Board reviewed and approved thestudy.
6 Pertinent history, demographics, laboratory find-ings, and outcomes were recorded. patients with a primaryadmission for AC were identified based on ICD-9-CMdiagnostic and procedural codes ( , , , , , ). From this cohort, patients with aprimary procedure code CCT , , or werequeried. All operative notes were reviewed to confirm in-tent and operative strategy. Operations beginning laparo-scopically and then switched intraoperatively to an openprocedure were defined as open conversion (CONV). Par-tial cholecystectomy procedures (n 5) were included inthe LC group, as these procedures were performed lapa-roscopically and resulted in similar surgical with missing data, incomplete operative notesand documents, and metastatic gastrointestinal cancerwere characteristics and demographics were com-pared among patients who received each treatment.
7 Agewas maintained as a continuous variable. Self-definedrace was divided into white, black, Hispanic, and comorbidities were recorded by reviewingeach patient s medical record for the presence of 9 con-ditions associated with adverse outcomes in hospitalizedpatients at the time of hospital admission. These comor-bidities were atrial fibrillation, coronary artery disease,previous myocardial infarction, chronic renal insuffi-ciency, congestive heart failure, hypertension, diabetesmellitus type 1 or 2, cirrhosis, and COPD. Diagnosticimaging and relevant findings were recorded for eachpatient. Laboratory values on admission included WBC,total bilirubin, alkaline phosphatase, aspartate amino-transferase, and mortality was defined as any death duringthe hospital stay. Major complications (after CCT place-ment, surgery, or in follow-up) were defined as requiringreadmission and identified by reviewing all inpatient andoutpatient notes for CCT-related andpostoperative-related is-sues.
8 Complications were categorized as follows: bile leak,bile duct injury, retained stone, bleeding, wound infection,urinary tract infection, pneumonia, subhepatic fluid col-lection, in-hospital myocardial infarction, and analysisFor patient-level data, means and SDs were calculated forcontinuous variables. SAS (SAS Institute)was used to analyze data. patients and outcomes wereanalyzed after being stratified by admission year andoperation performed. All analyses performed were uni-variate the 185 patients who received a CCT during their hos-pital stay, 144 (78%) were placed by radiology (pCCT) and41 (22%) were placed surgically (sCCT). Surgical consul-tation was obtained in all cases of CCT placement. Four-teen surgeons placed sCCT, with a median of 1 tube placedby each surgeon (range 1 to 15).
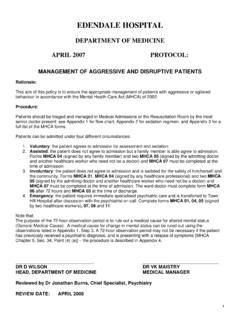
9 The 41 sCCTs were ini-tially planned as LCs but were converted to CCT place-ment during surgery for a variety of reasons, includingadhesions, severe inflammation, and edema. During thestudy period, the number of CCTs placed annually in-creased (Fig. 1). Median hospital stay was 5 days, and me-Abbreviations and AcronymsAC acute cholecystitisCCT cholecystectomy tubeCONV open conversionLC laparoscopic cholecystectomyOC open cholecystectomypCCT percutaneously placed Cholecystostomy tubesCCT surgically placed Cholecystostomy tube197 Vol. 214, No. 2, February 2012 Cherng et alCholecystostomy Tubes in Acute Cholecystitisdian length of stay between CCT placement and dischargewas 4 days (range 1 to 76 days).DemographicsTable 1summarizes the demographics of the the 185 patients who received a CCT during theirhospital stay for AC, the median age was 71 years old (range21 to 99 years old) and were majority ofpatients were of white race (n 156; ).
10 Sixty-four( ) of the patients had earlier abdominal majority of patients (n 149; 80%) had at least 1comorbidity, with a mean number of comorbidities(median 1). The maximum number of comorbidities was7(n 2). Hypertension was most common, followed bycoronary artery disease and diabetes mellitus type was diagnosed based on clinical and radiologicalfindings. Diagnostic imaging results are shown inTable was the imaging technique of choice andwas used in 116 patients and CT was used in 63 hundred and thirty-two patients ( ) had gall-stones, 114 ( ) showed gallbladder wall thickening,and 101 ( ) had evidence of pericholecystic laboratory values were collected, including WBCand bilirubin, alkaline phosphatase, aspartate aminotrans-ferase, and albumin levels (Table 2).CCT OutcomesOf 185 patients , the majority (n 105; ) even-tually underwent a subsequent cholecystectomies by 20 Figure of Cholecystostomy Tubes placed per year atUMass of procedures performed for removal of gall-bladder after placement of percutaneous or surgical cholecystos-tomy tube.