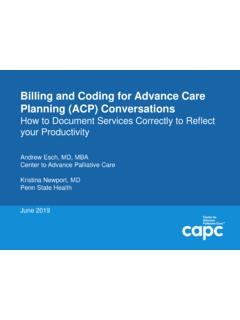
Transcription of Work Relative Value Units (wRVU) Table (2020) - Palliative ...
1 Work Relative Value Units (wRVU) Table (2020) - Palliative Care and HospiceInpatientInitial (min)99221 (30m)99222 (50m)99223 (70m) (15m)99232 (25m)99233 (35m) 99201 (10m)99202 (20m)99203 (30m)99204 (45m)99205 (60m) (5m)99212 (10m)99213 (15m)99214 (25m)99215 (40m) 99341 (20m)99342 (30m)99343 (45m)99344 (60m)99345 (75m) (15m)99348 (25m)99349 (40m)99350 (60m) 99304 (25m)99305 (35m)99306 (45m) Subsequent99307 (10m)99308 (15m)99309 (25m)99310 (35m) Annual99318 (30m) 99324 (20m)99325 (30m)99326 (45m)99327 (60m)99328 (75m) (15m)99335 (25m)99336 (40m)99337 (60m) ServiceFace-to-Face (add-on)Outpt (face-to-face)99354 (30-74m extra)99355 (76-105m) Inpt (unit/floor)99356 (30-74m extra)99357 (76-105m extra) (Not for hospice)Any setting99358 (31-75m)99359 (76-105m) Care PlanningAny setting99497 (16-45m)99498 (46-75m) Management (Not for Hospice)CM InitiationG0506 Chronic CM99490 (20m stafftime in a month) G2058 (add/l 20m;max 2 per month) CCM99487 (60m)99489 (90m+) Principal CMG2064 (30mMD/DO/QHP*) G2065 (30m staff) :# Significant changes are planned for Office & Prolonged svcs CPT codes reported, time needed, documnt'n required, and wRVUs in January 2021.
2 # Though Medicare will not, if your insurer pays consult codes (Outpt 99241-5; Inpt 99251-5), these codes have higher wRVUs than above.# All of these codes are billable for hospice patients except Non-F2F Prolonged Codes and Care Management Codes.# These are work RVUs only. Total RVUs include practice expense and malpractice expense RVUs as well.# RVU information comes from the Medicare Fee Schedule Lookup, shortened at *QHP = Qualified Healthcare ProviderInpatient Billing from 1995 Medicare Highmark Audit Tool Risk Time-based billing: I spent _____ minutes in Admits/Medicare Consult Inpt Consult (Not M care) Follow-up the care of this patient, >50% in Level 1 30 min Level 3 55 min Level 1 15 min counseling and care coordination.
3 Level 2 50 min Level 4 80 min Level 2 25 min Prolonged service: include Time in / Time out Level 3 70 min Level 5 110 min Level 3 35 min ACP (99497 16-45min; +99498 46-75min) E&M Initial Consult (HIGH): - 4 point HPI - 10 point ROS - PMFSH (all 3) - 8 system Exam - 2 of 3 High-level MDM: - 4 points Dx - 4 points data - High Risk E&M Follow-up Visit(HIGH): - Either 4 point HPI and 2 point ROS - OR 8 system Exam - 2 of 3 High-level MDM: - 4 points Dx - 4 points data - High Risk Special ReportTop 10 Tips for Using Advance Care Planning Codesin Palliative Medicine and BeyondChristopher A. Jones, MD,1,2 Jean Acevedo, LHRM, CPC, CHC, CENTC,3 Janet Bull, MD, MBA,4and Arif H.
4 Kamal, MD, MBA, MHS5,6 AbstractAlthough recommended for all persons with serious illness, advance care planning (ACP) has historically beena charitable clinical service. Inadequate or unreliable provisions for reimbursement, among other barriers, havespurred a gap between the evidence demonstrating the importance of timely ACP and recognition by payers forits the first time, healthcare is experiencing a dramatic shift in billing codes that support increasedcare management and care coordination. ACP, chronic care management, and transitional care managementcodes are examples of this newer recognition of the Value of these types of services .
5 ACP discussions are anintegral component of comprehensive, high-quality Palliative care delivery. The advent of reimbursementmechanisms to recognize these services has an enormous potential to impact Palliative care program sustain-ability and growth. In this article, we highlight 10 tips to effectively using the new ACP codes reimbursableunder Medicare. The importance of documentation, proper billing, and nuances regarding coding is :advance care planning; billing and coding; community-based Palliative care; inpatient palliativecare; outpatient Palliative care; revenueIntroductionAcore componentof high-quality Palliative care (PC)delivery is facilitation of regular advance care planning(ACP) discussions.
6 The National Hospice and PC Organiza-tion define ACP as making decisions about the care youwould want to receive if you become unable to speak foryourself. ACP also includes sharing care options for patientsdiagnosed with a serious illness, permitting patients to sharevalues and preferences for care with loved ones who will act assurrogates, and, sometimes, completing advance directive(AD) paperwork to put those wishes in ,ACP constitutes a longitudinal and dynamic process that re-quires thoughtful, regular, and often time-intensive conversa-tions between patients, their loved ones, and major barrier to widespread facilitation of ACP by cli-nicians has been lack of recognition by payers through ap-propriate reimbursement.
7 Efforts at increasing completion ofAD in the community3and skilled nursing facility settings4have had limited success but have not led to widespread,sustained increases in AD completion. As would be expected,when ACP processes are supported by project or grantfunding only and not routine reimbursement from payers,regular adoption of ACP is often not realized outside of re-search settings. As many begrudgingly remember, an attemptto include payment for ACP in 2009s Patient Protection andAffordable Care Act was derided as death panels 5and theprovision was dropped from the final several years of continued requests by healthcare andpatients rights groups to pay providers for ACP discussionswith their patients, the Centers for Medicare and MedicaidServices (CMS) reversed course.
8 On October 30, 2015, CMSannounced a proposal that supports patient- and family-centered care for seniors and other Medicare beneficiaries byenabling them to discuss ACP with their providers. 7 Yet,payers did not provide robust guidance for how cliniciansshould implement these changes. In this article, we willpresent 10 tips to compliantly provide ACP services toMedicare patients and offer insight into billing for theseservices. While the information we provide is intended for anaudience of PC practitioners, the information is applicable toproviders of all Line Health, Radnor, Medical Center, Wynnewood, Consulting, Inc.
9 , Delray Beach, Seasons Compassion for Life, Flat Rock, North Palliative Care, Durham, North Cancer Institute, Durham, North OF Palliative MEDICINEV olume 19, Number 12, 2016 Mary Ann liebert , : 1: Medicare has adopted CPT codes 99497 and99498 to reimburse for ACP and will utilize CPTs broaddefinition of s definition of ACP was adopted from theAmerican Medical Association s Current Procedural Ter-minology (CPT) is defined within CPT asa face-to-face service between a physician or other qualifiedhealthcare professional and a patient, family member, orsurrogate in counseling and discussing AD, with or withoutcompleting relevant legal forms.
10 An AD is a documentappointing an agent and/or recording the wishes of a patientpertaining to his/her medical treatment at a future time shouldhe/she lack decisional capacity at that time. 8 CPT code 99497 pays for ACP, including the explanationand discussion of AD such as standard forms (with comple-tion of such forms, when performed), by the physician orother qualified healthcare professional, first 30 minutes, face-to-face with the patient, family member(s), and/or surrogate and code 99498 reimburses for each additional 30 99498 is an add-on code and so can only be used alongwith code is important to understand that CPT guidelines state thatcertain time-based codes, ACP codes included, may be usedwhen 1 minute more than the midpoint of the code time isreached.