
BERT Claim Form
BERT Claim Form Please return this completed form to: Email: claims@bert.com.au | Fax: 07 3832 3799 | Post: BERT, PO Box 805, SPRING HILL QLD 4004 Office: Level 1, 35 Astor Terrace, SPRING HILL QLD 4000 Please mark the applicable claim type (x) Redundancy Leaving the Industry Retirement
Download BERT Claim Form

Information
Domain:
Source:
Link to this page:
Documents from same domain
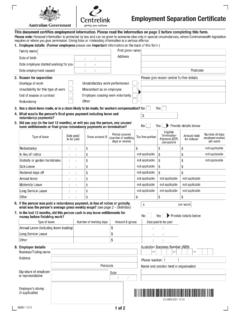
Employment Separation Certificate
www.bert.com.auEmployment Separation Certificate SU001.1012 (for Certificate, see page 1) Information for Former Employees If you do not have another job to go to and you want to claim a Centrelink payment you will need to:
Related documents

www.elaflex.de
www.elaflex.de328 AUSSEN DURCHMESSER STEIGUNG INNEN DURCHMESSER GEWINDEART/ GEWINDEGRÖSSE GEWINDE NORM Outer Diameter Pitch Inner Diameter Type / …

Form Working Holiday visa 1263 Employment …
www.homeaffairs.gov.auCOMMONWEALTH OF AUSTRALIA, 2018 1263 (Design date 03/18) - Page 1 Working Holiday visa Employment verication Form 1263 epartment of ome Affairs About this form

CLASS P - LANGUAGE AND LITERATURE
www.loc.govLIBRARY OF CONGRESS CLASSIFICATION OUTLINE . CLASS P - LANGUAGE AND LITERATURE (Click each subclass for details) Subclass P Philology. Linguistics

聖保祿樂靜院 團體申請表 - srspc.org.hk
www.srspc.org.hk聖保祿樂靜院 個人申請表 申請人姓名 : (先生/女士) 身份證號碼: (首字母及3位數字)住址 : 電郵地址 : 聯絡電話 :

Parcel ID (Tax Map Key) - realpropertyhonolulu.com
www.realpropertyhonolulu.comreal property tax exemption for kuleana land roh section 8-10.32 last name , first name middle initial phone number date of birth email address last name , …