
CASHLESS AUTHORIZATION REQUEST NOTE
DECLARATION BY THE PATIENT / REPRESENTATIVE 1. I agree to allow the hospital to submit all original documents pertaining to hospitalization to the Insurer/T.P.A after the discharge.
Download CASHLESS AUTHORIZATION REQUEST NOTE

Information
Domain:
Source:
Link to this page:
Documents from same domain
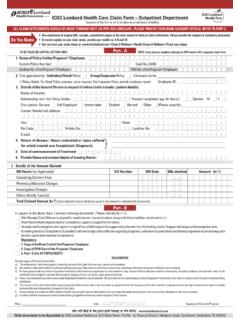
ICICI Lombard ICICI Lombard Health Care Claim …
www.icicilombard.comICICI Lombard Health Care DDMMYY D D D D M M Y Y M M Y Y DDMMYY Y N Y N Y N Y N 7. Details of the Amount Claimed Bill Heads (as Applicable) Bill Number Bill Date Bills attached Amount (In `)
Out Patient Department (OPD) Cashless Card ... - ICICI Lombard
www.icicilombard.com2 Cashless OPD card iHealth Card A first of its kind concept Cashless OPD valid for 1 year No copay, sublimit or deductions For Employees (E), Employee-Spouse-Children (ESC) and Employee- Spouse-Children-Parents (ESCP) The card allows cashless GP & Specialist consultation along with Diagnostics (all pathology related, Sonography and ECG) in select

013511PW-SC International Travel Insurance Policy Wording
www.icicilombard.comsubsequent premiums, as set out in the Policy Schedule with all its Parts, and further, ... roller hockey, rugby, ski acrobatics, ski doo ski jumping, ski racing, sky diving, small bore target shooting, speed trials/ time trials, triathlon, water ski jumping, weight lifting, wrestling and activities of similar nature. ...

KEY INFORMATION SHEET - ICICI Lombard
www.icicilombard.comSub Limit (a) Cataract, where sub-limit of Rs.20,000/- is applicable per eye per Policy year for Plans with Sum Insured up to 5Lacs. Sub limit of Rs.1,00,000 per eye per Policy year will be applicable for cataract treatment for plans with Sum Insured above Rs.5Lacs Part II of the schedule Clause 3.2 8
Complete Health Insurance Brochure - ICICI Lombard
www.icicilombard.comAn Additional Sum Insured of 10% of Annual Sum Insured provided on each renewal for every claim free year up to a maximum of 50%. In case of a claim under the policy, the accumulated Additional Sum Insured will be reduced by 10% of the Annual Sum Insured in the following year. Option of choosing 1 or 2 year policy period under various plans ...
Related documents

C-4.2 Doctor's Progress Report - Government of New York
www.wcb.ny.govImportant: Form C-4 AUTH should be used to request any special medical service over $1000 or for those services requiring pre-authorization pursuant to the Medical Treatment Guidelines for the back, neck, knee and shoulder. 4.

Real Time Release Testing guideline
www.ema.europa.euThe introduction of RTRT requires pre-authorization by the competent authority. In general the documentation submitted for a new market authorization or a variation should address only those quality aspects that are specific for the medicinal product. Site specific quality aspects not specific to

Durable Medical Equipment Requiring Pre-Authorization
provider.carefirst.comDurable Medical Equipment Which Require Pre-Authorization Service Service description K0831 POWER WHEELCHAIR, GROUP 2 STANDARD, SEAT ELEVATOR, CAPTAINS CHAIR, PATIENT WEIGHT CAPACITY UP TO AND INCLUDING 300 POUNDS K0835 POWER WHEELCHAIR, GROUP 2 STANDARD, SINGLE POWER OPTION, SLING/SOLID SEAT/BACK,

SAMPLE LETTER OF APPEAL TEMPLATE To be considered …
www.cardiovascular.abbottdenied claim or pre-authorization . Instructions for completing the sample appeal letter: 1. Please customize the appeal letter template based on the medical appropriateness. Fields required for customization are in RED. 2. It is important to provide the most complete information to assist with the appeal of a prior authorization denial. 3.
Florida DBPR Examination Information Bulletin Computer ...
iccsafe.orgJul 10, 2020 · Florida DBPR candidates that would like to receive pre-authorization should contact DBPR at 1-850-487-1395. Pre-authorized Florida DBPR candidates must pass both the ICC technical examination and the Build-ing Code Administrators and Inspectors Florida Principles and Practice Licensure Examination before being issued a Florida license.