
NYL Disclosure Authorization - Cigna
Disclosure Authorization. Claimant’s Name: NOTE: This authorization is designed to comply with the Health Insurance Portability and Accountability Act of 1996 ("HIPAA") and relates to information necessary to administer benefits and services under Employer’s employee health and welfare plan(s) ("the
Download NYL Disclosure Authorization - Cigna

Information
Domain:
Source:
Link to this page:
Documents from same domain

My payment preferences Manage your account online at ...
www.newyorklife.comAddress No PO boxes please STREET APT. CITY STATE ZIP STEP 5B Please only complete if the bank account holder named above (the payer) is not the policy owner. Helpful tip: provide the Designated Payer’s information below and indicate payer type in the signature section below. STEP 6B Please only complete if you are a Designated Payer.
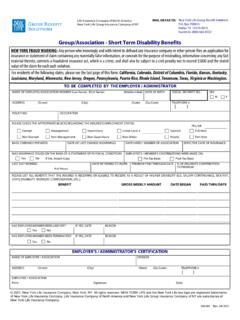
Group/Association - Short Term Disability Benefits
www.newyorklife.cominsurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to a civil penalty not to exceed $5000 and the stated value of the claim for each such violation.

My beneficiary changes - New York Life
www.newyorklife.com21131 11/2020 2 Q A custodian is the person named to manage a minor’s property under the Uniform Transfers/Gifts to Minors Act (UTMA/UGMA). Remem ber, each minor needs a custodian—the custodian can be the same person for each minor. Q UTMA/UGMA state will be the minor’s state of residence listed in Step 2, unless a different state is listed below.

Disability Claim Policies & Procedures
www.newyorklife.comThe Policies and Procedures disclosed to customers include the guidelines generally applicable to processing their claim. Depending upon the experience of the Claim Manager and/or the issues presented in any given claim, the Claim Manager may or may not have needed to actually review any part of these Policies and Procedures during claim ...

Certification of Employee Health Care Provider
www.newyorklife.comThe Genetic Information Nondiscrimination Act of 2008 (GINA), and, where applicable, the California Genetic Information Nondiscrimination Act of 2011 (CalGINA), prohibits employers and other entities covered by GINA Title II, and where applicable CaGl INA, from requesting or requiring genetic information of employees or their

Frequently Asked Questions Concerning Death Benefit …
www.newyorklife.comA Death Benefit Proceeds form will be sent to the beneficiary(s) on record. It can also be obtained by calling (800) 695-9873 (8 a.m. - 7 p.m. ET). Or you can report a death online at www.newyorklife.com and a Death Benefits Proceeds form …

Policy loan request - New York Life
www.newyorklife.comFor residents of Connecticut: We are required to withhold state income tax from the taxable portion of your payments, unless you provide us with a properly completed Form CT-W4P and you claim an exemption from withholding. An exemption …
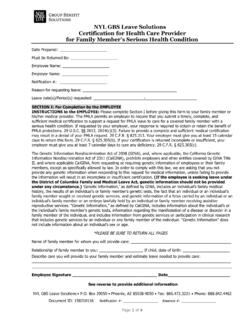
Certification of Family Health Care Provider
www.newyorklife.comSignature of Health Care Provider Date NYL GBS Leave Solutions • P.O. Box 703509 • Dallas, TX 75370 • Fax: 866.931.5095 • Phone: 888.842.4462 Certification of Health Care Provider

ELECTRONIC FUND TRANSFER (EFT) AUTHORIZATION FORM
www.newyorklife.comunderstand that the EFT service is only available for personal accounts, not business or corporate. I also understand that the EFT service will stay in effect until I notify the Company of cancellation on the EFT service authorization form.

Request for Federal Income Tax Withholding From Sick Pay
www.newyorklife.comare already required to withhold federal income tax from. return. For exceptions and details, see Pub. 505, Tax Withholding. sick pay. Note: If you receive sick pay under a collective bargaining agreement, see your union representative or employer. Definition. Sick pay is a payment that you receive: • Under a plan to which your employer is a ...
Related documents

IN-HOME SUPPORTIVE SERVICES (IHSS) PROGRAM …
file.lacounty.govIN-HOME SUPPORTIVE SERVICES (IHSS) PROGRAM PROVIDER ENROLLMENT FORM INSTRUCTIONS: † Use black or blue ink to fill out. Print information clearly. † Fill out, sign and return this form in person to the office or location designated by the county. Bring original federal or state government-issued identification and your original Social Security card when returning …

New York State Medicaid Enrollment Form
www.emedny.orgEnrollment Form Thank you for your interest in enrolling with the New York State Medicaid Program. As a Medicaid provider, you agree to comply with the rules, regulations and official directives of the Department including, but not limited to , Part 504 of 18 NYCRR (i.e., Title 18). Title 18 can be found by choosing the Laws and

New York State Medicaid Enrollment Form
www.emedny.org2. A Medicaid Managed Care Network provider. If you will also provide medical services to patients, or as an attending provider will submit a separate claim to Medicaid for your service, do not complete this form. Visit www.eMedNY.org and complete the enrollment form appropriate for your license/certification. Consider printing the