Authorization To Release School Information
Found 8 free book(s)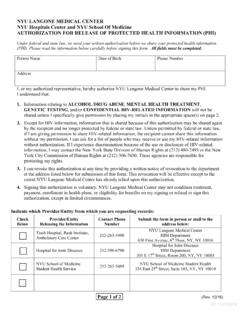
AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH …
med.nyu.eduNYU Hospitals Center and NYU School Of Medicine . AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION (PHI) Under federal and state law, we need your written authorization before we share your protected health information (PHI). Please read the information below carefully before signing this form. All fields must be completed.

Authorization for Release of Information - IHACares
www.ihacares.comTransfer from pediatric to adult doctor Legal School Insurance Change (Non-par) Workers Compensation Medical Care Billing Information Other (please specify): _____ 1. I understand that this authorization will expire 60 days after I have signed the form. 2.

AUTHORIZATION FOR RELEASE/REQUEST OF INFORMATION
www.childrensmn.orgstop this authorization, I must do so in writing to Health Information Management. I understand that stopping this authorization will not apply to information that has already been released or disclosed.4. • I understand that authorizing the release of this health information is voluntary. I can refuse to sign this authorization.
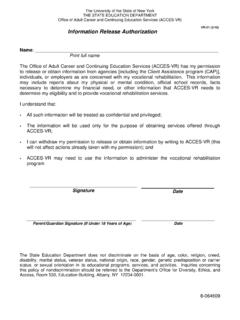
Information Release Authorization
www.acces.nysed.govInformation Release Authorization . Name: _____ Print full name . The Office of Adult Career and Continuing Education Services (ACCES-VR) has my permission to release or obtain information from agencies [including the Client Assistance program (CAP)], individuals, or employers as are concerned with my vocational rehabilitation. This information

AUTHORIZATION TO DISCLOSE PROTECTED HEALTH …
eforms.comited to, all records and other information regarding health history, treatment, hospitalization, tests, and outpatient care, and also educational records that may contain health information. As indicated on the form, specific authorization is required for the release of information about certain sensitive conditions, including:

AUTHORIZATION TO RELEASE/OBTAIN/EXCHANGE …
www.seattlechildrens.orgA general authorization for the release of medical or other information is NOT sufficient for this purpose. The federal rules restrict any use of the information to criminally investigate or prosecute any alcohol or drug abuse patient.

FORM APPROVED: OMB NO. 0917-0030 DEPARTMENT OF …
www.ihs.govAUTHORIZATION FOR USE OR DISCLOSURE OF PROTECTED HEALTH INFORMATION. COMPLETE ALL SECTIONS, DATE, AND SIGN. I. I, (Name of Patient), hereby voluntarily authorize the disclosure of information from my health record. II. The information is to be disclosed by: NAME OF FACILITY ADDRESS. CITY/STATE. And is to be provided to: NAME …

Transcript Request Service & Release Forms
www.columbiasouthern.eduTranscript Request Service & Release Forms P.O. Box 3110 | 21982 University Lane | Orange Beach, AL 36561| 800.977.8449 | Fax 251.224.0540 Columbia Southern Universit y Page 1 of 2