Search results with tag "Authorization for release"

#2687, Authorization for Release of FBI Information
dsps.wi.govGeneral of the United States, or other authorized authorities. Examples include but are not limited to 5 U.S.C. 9101; ... #2687, Authorization for Release of FBI Information Subject #2687, Authorization for Release of FBI Information Keywords

OCA Official Form No.: 960 AUTHORIZATION FOR RELEASE …
nycourts.govInstructions for the Use of the HIPAA-compliant Authorization Form to Release Health Information Needed for Litigation This form is the product of a collaborative process between the New York State

OCA Official Form No.: 960 AUTHORIZATION FOR RELEASE …
www.nycourts.govof the HIPAA-compliant Authorization Form to Release Health Information Needed for Litigation This form is the product of a collaborative process between the New York State Office of Court Administration, representatives of the medical provider community in New York, and the bench and bar, designed to produce a standard official form that
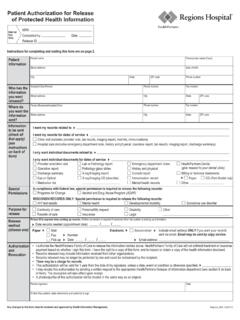
Patient Authorization for Release of Protected Health ...
www.healthpartners.com• This authorization will be valid for 1 year from the date of my signature, unless a date, event or condition is otherwise specified. • I may revoke this authorization by sending a written request to the appropriate HealthPartners Release of Information department (see section 8 on back of form). The revocation will take effect upon receipt.
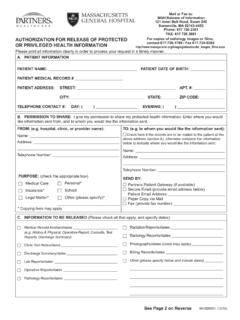
Mail or Fax to: MGH Release of Information 121 Inner Belt ...
www.massgeneral.orgA. PATIENT INFORMATION PATIENT NAME: PATIENT DATE OF BIRTH: PATIENT MEDICAL RECORD # PATIENT ADDRESS: STREET: APT. ... AUTHORIZATION FOR RELEASE OF PROTECTED OR PRIVILEGED HEALTH INFORMATION 84182MGH (12/16) ... Yes Confidential Communications with a Licensed Social Worker
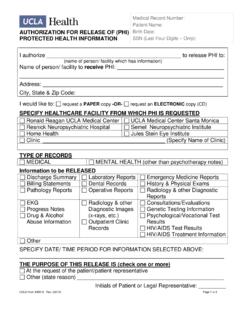
Medical Record Number: Patient Name: AUTHORIZATION …
www.uclahealth.orgAUTHORIZATION FOR RELEASE OF (PHI) PROTECTED HEALTH INFORMATION SSN (Last Four Digits UCLA Form #30910 Rev. (02/14) Page 1 of 2
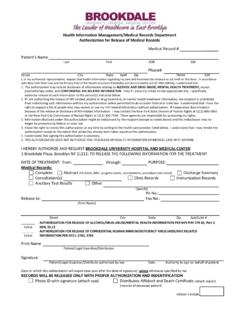
Health Information Management/Medical Records …
www.brookdalehospital.orgHealth Information Management/Medical Records Department Authorization for Release of Medical Records . Medical Record # Patient’s Name . Last First DOB SS#

Authorization for Release of Protected Health Information
www.fvfiles.comDirections for Completing the Authorization for Release of Protected Health Information Form Fill out the entire form neatly. Please print. Please note that blank items on this form may cause major delays in processing your request. Complete this form as fully as possible. Allow a …

AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH …
www.dhcs.ca.govAUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION TO THIRD PARTIES File Number: _____ By completing this form you are authorizing the California Department of Health Care Services to release your protected health information identified herein to the persons or entities identified herein.

AUTHORIZATION FOR RELEASE OF INFORMATION (for Use …
ukhealthcare.uky.eduthis Authorization, however, Facility may condition the provision of health care that is solely for the purpose of creating protected health information for disclosure to a third party on my signing this Authorization, and Facility may condition the provision of research-related treatment on my signing this Authorization.
AUTHORIZATION FOR RELEASE OF HEALTH INFORMATION
www.ucsfhealth.orgDate Time Relationship to Patient (Parent, Guardian, Conservator, Patient Representative) Requested format: ☐ Paper ☐ CD ☐ Jump Drive DATE: PATIENT NAME: BIRTHDATE: ID VERIFICATION (TYPE): ID VERIFIED BY: AUTHORIZATION FOR RELEASE OF HEALTH INFORMATION 756-020Z i (Rev. 04/21) MEDICAL RECORD COPY AUTHORIZATION FOR …

AUTHORIZATION FOR RELEASE/REQUEST OF INFORMATION
www.childrensmn.orgAUTHORIZATION FOR RELEASE/REQUEST OF INFORMATION *ROI* Operative Report Laboratory Report X-Ray Report Other:_____ Consultation Testing Records X-Ray Image(s) Immunizations Mental Health Record Clinic Visit How to upload to MyChildren’s portal Print and complete this form. 2.
AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH …
med.nyu.edu2. Except for HIV information, information that is shared because of this authorization may be shared again by the recipient and no longer protected by federal or state law. Unless permitted by federal or state law, if I am giving permission to share HIV-related information, the recipient cannot share this information without my permission.

AUTHORIZATION FOR RELEASE OF PROTECTED OR …
www.partners.orgAUTHORIZATION FOR RELEASE OF PROTECTED OR PRIVILEGED HEALTH INFORMATION D. Please check YES to indicate if you give permission to release the following information if present in your record:

AUTHORIZATION FOR RELEASE OF PROTECTED OR …
www.partners.orgDFCI or BWH receives a request for the release of the other hospital’s records, the request will be forwarded to the appropriate hospital to respond to the request. See Page 2 on Reverse 84182BWH (9/16) A. PATIENT INFORMATION PATIENT NAME: PATIENT DATE OF BIRTH: PATIENT MEDICAL RECORD # PATIENT ADDRESS: STREET: APT. #: CITY: STATE: ZIP …