Health authorization
Found 10 free book(s)
LOS ANGELES COUNTY DEPARTMENT OF MENTAL HEALTH ...
lacdmh.lacounty.govlos angeles county department of mental health authorization for use or disclosure of protected health information mh 602 (09/2016) page 1 of 2

California Prior Authorization Requirements - Health Net
www.healthnet.comCalifornia Prior Authorization Requirements Health Net of California, Inc. and Health Net Life Insurance Company (Health Net) Direct Network1 HMO (including CommunityCare HMO), Point of Service (POS) Tier 1 and Medicare Advantage (MA) HMO

NH Authorization to Disclose Protected Health or Billing ...
www2.novanthealth.orgAuthorization to Disclose Protected Health or Billing Information Patient Information: I give permission to release the health information of: (One patient per form)

Texas Standard Prior Authorization Request Form for Health ...
www.bcbstx.comTitle: Texas Standard Prior Authorization Request Form for Health Care Services Author: Texas Department of Insurance Keywords: prior authorization request form, NOFR001, SB 1216

OCA Form No. 960 - Authorization for Release of Health ...
www.nycourts.govInstructions for the Use of the HIPAA-compliant Authorization Form to Release Health Information Needed for Litigation This form is the product of a collaborative process between the New York State

Organized Health Care Arrangement Request
www.uchospitals.eduSend your Request and Authorization to Copy Health Information to the UC Organization that maintains your records. UCMC Medical Records Dept: Phone (773) 702-1637; Fax (773) 702-7591
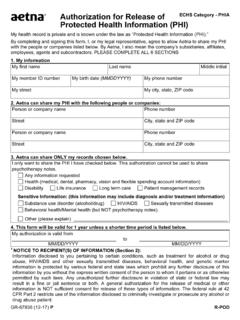
Authorization for Release of Protected Health Information ...
www.aetna.comGR-67938 (12-17) P Authorization for Release of Protected Health Information (PHI) ECHS Category - PHIA My health record is private and is known under the law as “Protected Health Information (PHI).”

Authorization for Release of Protected Health Information
www.fvfiles.com521125 – REV 08/18 INFORMATIONAL PAGE ONLY Directions for Completing the Authorization for Release of Protected Health Information Form Fill out the entire form neatly.

AUTHORIZATION FOR DISCLOSURE OF PROTECTED HEALTH …
www.ketteringhealth.orgAUTHORIZATION FOR DISCLOSURE OF PROTECTED HEALTH INFORMATION. Patient Name: Date of Birth: Phone Number: Social Security #: Date of Treatment:

REQUEST FOR PRIOR AUTHORIZATION FAX ... - SANTÉ …
www.santehealth.netREQUEST FOR PRIOR AUTHORIZATION FAX (559) 224-2405 or (559) 224-9746 PHONE (559) 228-5400 or (800) 652-2900 O Aqua Therapy O Intensity Modulated Radiation Therapy (IMRT)
Similar queries
ANGELES COUNTY DEPARTMENT OF MENTAL HEALTH, Angeles county department of mental health authorization, Protected health information, Prior Authorization Requirements, Health Net, Prior Authorization Requirements Health Net, AUTHORIZATION, Health, Texas Standard Prior Authorization Request Form, HIPAA, Organized Health Care Arrangement, Authorization for Release of Protected Health Information, AUTHORIZATION FOR DISCLOSURE OF PROTECTED HEALTH, AUTHORIZATION FOR DISCLOSURE OF PROTECTED HEALTH INFORMATION