Name Holder Account
Found 7 free book(s)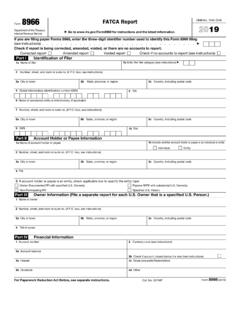
2021 Form 8966 - IRS tax forms
www.irs.govName of account holder or payee. 1b. Indicate whether account holder or payee is an individual or entity. Individual. Entity2 . Number, street, and room or suite no. (if P.O. box, see instructions) 3a. City or town. 3b. State, province, or region. 3c. Country, including postal code . 4 . TIN. 5 . If account holder or payee is an entity, check ...

New Holder/Recipient Information - Computershare
www.computershare.comEnter the name of the current holder (s), the name of the issuer of the securities and the certificate or account number. This information is detailed on the certificate or the securityholder statement/advice. • If holdings to be transferred include securities held in …
Fax To: 518-560-5102 Identity Proofing Only
info.nystateofhealth.ny.govas DOB and SSN. If the account number is not available, write the Client Name DOB andon each page of the fax . Separate faxes must be sent for each primary account holder. Submission of incomplete fax coversheets, identity proofing forms, or documents may cause a …
AUTHORIZATION FOR PAYOFF AND TITLE PROCESSING
www.sc.toyotafinancial.comIf no name is indicated, the certificate of title will be mailed to the account holder/customer. Customer Signature: Co-Buyer Signature: Date: Date: I/We agree that any facsimile transmission of this document stored by LFS in electronic or paper form shall constitute an original for all purposes of this authorization.

Account Holder Name Change Request - Chase.com
www.chase.comAccount Holder Former Name. Account Number. Exemption from FACTA Reporting Code (if any) Social Security or Tax ID Number (required) According to the IRS Form W-9 instructions, if you are only submitting this form for an account you hold in the United States, you may leave the Exemption from FACTA Reporting code field blank. 1. Tell Us About ...

Account authorization form - HealthEquity
resources.healthequity.comSignature of account holder Date If at any time you need to alter this authorization form, please contact HealthEquity at 866.346.5800. Name of authorized individual …

Seller Buyer Name Name Co-owner Co-owner Seller’s …
www.hfcu.orgPurchase Agreement Seller Buyer Name_____ Name_____ Co-owner_____ Co-owner_____