Provider Appeal Request
Found 9 free book(s)
Practitioner and Provider Compliant and Appeal Request
www.aetna.comPractitioner and Provider Complaint and Appeal Request NOTE: Completion of this form is mandatory. To obtain a review submit this form as well as information that will support your appeal…
PLEASE PRINT OR TYPE SECTION 1. IDENTIFYING …
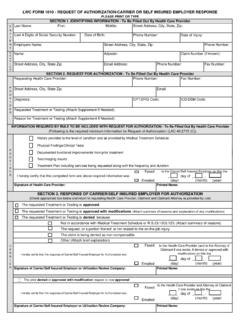
www.laworks.netFaxed Emailed Faxed Emailed Faxed Emailed C A R R I E R P R O V Appeal of Suspension to Medical Services Section by Health Care Provider I hereby certify that this First Request and accompanying Form 1010A was _____ day of _____ , _____ (day) (month) (year)

PROVIDER APPEAL REQUEST FORM - lmchealthplans.com
www.lmchealthplans.com07/2016 PROVIDER APPEAL REQUEST FORM This form should be used if you disagree with the outcome of your claims inquiry or have additional information which

Aetna Medicare Advantage Plan non -contract provider ...
www.aetna.comAetna Medicare Advantage Plan non -contract provider payment appeal process You have the right to appeal our payment denial by initiating the Medicare Managed

State of California Division of Workers’ Compensation ...
www.dir.ca.govDWC Form SBR-1 (Effective 2/2014) Page 1 State of California Division of Workers’ Compensation Provider’s Request for Second Bill Review

COLORADO ACCESS CLAIM APPEAL FORM
www.coaccess.comcoaess.o 1-800-511-5010 C COLORADO ACCESS CLAIM APPEAL FORM All fields are required. If information is missing, the appeal will not be processed and will be returned to the address

Texas Standard Prior Authorization Request Form for …
www.bcbstx.comTitle: Texas Standard Prior Authorization Request Form for Health Care Services Author: Texas Department of Insurance Keywords: prior authorization request form, NOFR001, SB 1216

Request for Claim Review Form
www.hcasma.orgMassachusetts Administrative Simplification Collaborative–Request for Claim Review V1.01 Request for Claim Review Form Today’s Date (MM/DD/YY): Health Plan Name:

Request for Claim Review Form
www.hcasma.orgThis guide will help you to correctly submit the Request for Claim Review Form. The information provided is not meant to contradict or replace a payer’s
Similar queries
Practitioner and Provider Compliant and Appeal Request, Provider, Appeal Request, Appeal, Request, PROVIDER APPEAL REQUEST FORM, Aetna, California Division of Workers’ Compensation, California Division of Workers’ Compensation Provider, Request for Second Bill Review, COLORADO ACCESS CLAIM APPEAL FORM, Texas Standard Prior Authorization Request Form, Request for Claim Review Form, Review Form