Reimbursement Requests
Found 7 free book(s)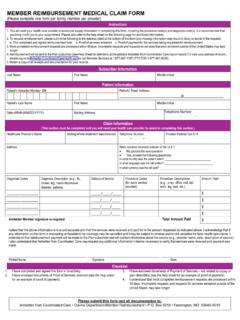
MEMBER REIMBURSEMENT MEDICAL CLAIM FORM
ambetter.coordinatedcarehealth.coma.This completed and signed reimbursement form b.Proof of services rendered c.Proof of payment for the services being requested for reimbursement 3.Most completed reimbursement requests are processed within 45 days. Incomplete requests and requests for services that were rendered outside of the United States may take longer.

Member Reimbursement Form for Medical Claims
wa.kaiserpermanente.orgReimbursement requests will be processed within 60 days of receipt. Itemized receipts, invoices, and proof of payment must be submitted, otherwise form may be sent back for lack of information. Submit all documents to: Claims Processing Kaiser P ermanente P .O. Box 30766 Salt Lake City, UT 84130-0766 Member Reimbursement Form for Medical Claims

REIMBURSEMENT APPLICATION - AAA
www.ace.aaa.comReimbursement requests cannot be processed with a photocopy or facsimile. • The receipt must be made out to a valid AAA member. • This application and your receipt must be postmarked within sixty (60) days of the service date. Please follow these instructions: Complete this application form fully. Please type or print legibly to expedite ...

0348-0004 REQUEST FOR ADVANCE OR REIMBURSEMENT …
www.sba.govexpenditure basis. All requests for advances shall be prepared on a cash basis. Enter the Federal grant number, or other identifying number assigned by the Federal sponsoring agency. If the advance or reimbursement is for more than one grant or other agreement, insert N/A; then, show the aggregate amounts. On a separate sheet, list each grant or
Advance Payment, Liquidation/ Reimbursement, and …
www.usaid.govRequests for advance payments may be submitted as follows: (1) Every 30 days covering a 30-day period; (2) Three requests may be submitted covering 30-day sub-periods of a 90-day period to be paid automatically every 30 days; or (3) One request for 90 days may be submitted to be automatically disbursed in 30-day equal increments.

CLAIMANT'S RECORD OF MEDICAL AND TRAVEL EXPENSES …
www.wcb.ny.govAND REQUEST FOR REIMBURSEMENT. CLAIMANT'S NAME . WCB CASE NO. SOCIAL SECURITY NO. In connection with the above workers compensation case, you are entitled to be reimbursed for (1) medications or supplies properly prescribed by your health care provider that you paid for yourself and for (2) fares, automobile

Reimbursement Claim Form - tasconline.com
www.tasconline.comReimbursement Claim Form Please complete this form to request reimbursement of expenses incurred by you and/or eligible dependents. Itemized documentation of each expense must be provided. For questions, contact Customer Care at 877‐933‐3539.