State Disability Claim
Found 7 free book(s)
DBL State Disability Claim Packet - NY, sny9457
www.standard.comsny 9457 3 of 6 (8/12) notice and proof of claim for disability benefits important: use this form only when the claimant becomes sick or disabled while employed or becomes sick or disabled within four (4) weeks after termination of employment.

SHORT TERM DISABILITY CLAIM FORM - Unum
forms.unum.comInstructions (continued) / Claim Fraud Statements CL-1104 (08/12) 3 SHORT TERM DISABILITY CLAIM FORM The Benefits Center P.O. Box 100158, Columbia, SC 29202-3158
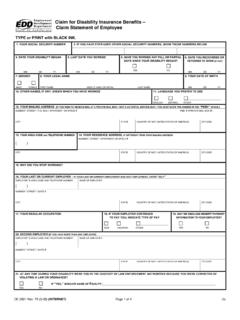
DE 2501 - Claim for Disability Insurance Benefits
www.heartinstitutehd.comDE 2501 Rev. 75 (3-05) (INTERNET) Page 1 of 4 CU Claim for Disability Insurance Benefits – Claim Statement of Employee TYPE or PRINT with BLACK INK. 1. YOUR SOCIAL SECURITY NUMBER 2.

New York State NOTICE AND PROOF OF CLAIM FOR …
www.wcb.ny.gov3. No-Fault motor vehicle accident (check box): No or personal injury involving third party (check box):. New York State NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS. Use this form if you became disabled . while employed

LONG TERM DISABILITY CLAIM FORM - Unum
forms.unum.comEMPLOYEE/INDIVIDUAL STATEMENT (PLEASE PRINT) A. Information About You Last Name Suffix First Name MI Date of Birth (mm/dd/yy) Social Security Number Gender The state in which you work

DISABILITY CLAIM FOR ACCIDENT & SICKNESS (A&S)/ …
www.isibenefits.comPage 4 of 4 A&S STD LTD UNI 5782 (07/05) eF Disability Claim Statement (Continued) Fraud Warning: If you are insured under a policy issued in one of the following states, or if you reside in one of the following states, one of the following state warnings may apply to you:

STATE OF CALIFORNIA Division of Workers' Compensation ...
www.dir.ca.govSTATE OF CALIFORNIA Division of Workers' Compensation Disability Evaluation Unit EMPLOYEE'S DISABILITY QUESTIONNAIRE Employee DEU Use Only. This form will aid the doctor in determining your permanent impairment or disability.