To Submit Claims
Found 6 free book(s)
Becoming a Medicaid Provider / Medicaid Claims
nj.govIn the Medicaid-based, fee-for-service system, in order to submit claims for services rendered, an agency must be a Medicaid (“Medicaid approved provider”). This is required whether agency is new an to the Division or has previously contracted with us. Agencies will only be reimbursed for services provided after Medicaid approval was received.

Cigna Dental eServices Electronic Claims Submission
www.cigna.comSubmit claims through a no cost web service; free transactions. Emdeon ®, Inmediata**, or other third-party vendor – Submit claims through a clearinghouse. NEA Fast Attach™ (nea-fast.com) – Submit X-rays and other attachments at a discount*. Find out how much money Visit the National EDI Council’s Return on

Registration Processing Times
www.copyright.govavailable to review claims. For example, claims take longer to process when applicants submit online claims but do not submit physical deposits when necessary, or when applicants do not fully respond to an examiner’s questions. The Office encourages applicants to refer to the Compendium of

Claims Filing Guidelines - Aetna
www.aetnabetterhealth.comClaims Filing Guidelines Claims Timely Filing Guideline . Plan Participating Providers ; Provider shall mail or electronically transfer (submit) the claim within ... When the Managed Care Plan is the secondary payer, the provider must submit the claim within : ninety (90) calendar days : after the final determination of the primary payer. ...
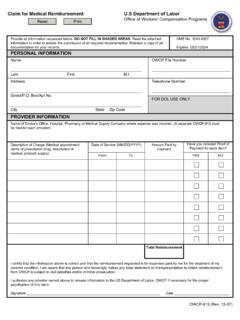
Claim for Medical Reimbursement U.S Department of Labor ...
www.dol.gov• Please submit a separate reimbursement claim for each provider where an out of pocket expense was incurred. • Please print clearly and legibly. Reference your OWCP file number on all documentation. Maintain a copy of the completed OWCP- …

SUBMIT YOUR WELLNESS BENEFIT REQUEST Complete all …
docs.usablelife.comIn signing below, I represent the statements I may have provided for claim review are true, complete and correct. I hereby authorize third persons,