Search results with tag "First last"
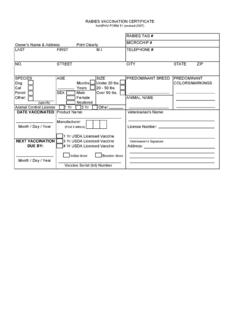
Owner's Name & Address Print Clearly LAST FIRST M.I ...
www.nasphv.orgLAST FIRST M.I. TELEPHONE # NO. STREET CITY STATE ZIP SPECIES AGE SIZE PREDOMINANT BREED PREDOMINANT ... 50 lbs. Ferret SEX Male Over 50 lbs. Other: Female ANIMAL NAME (specify) Neutered Animal Control License 1 Yr 3 Yr Other Manufacturer: (First 3 letters) License Number: 3 Yr USDA Licensed Vaccine Veterinarian's Signature

Complaint Form - New York State Department of Health
www.health.ny.govLast First MI Address Number & Street Name City State Zip Code Telephone ( ) – INFORMATION ABOUT THE PATIENT(S) ** You may add additional patient names on a separate sheet of paper. Patient(s) Name Last First MI Date of Birth / / Month Day Year DETAILS OF YOUR COMPLAINT

2018 Tomato Patch Registration Packet - kelseyatmccc.org
www.kelseyatmccc.orgTomato Patch 2018 Registration Form Student & Parent Information Student’s Full Name: Last First Parent’s/ Guardian’s Full Name: Last First Address:

Name: FIRST LAST - Skirmish
www.skirmish.comIf you are 17 or younger have legal guardian sign Name: First / Last. do hereby affirm and acknowledge that I am aware of and/or have been fully informed of the following:

Required Supervised Clinical Experience LCPC
health.maryland.govAPPLICANT'S NAME AND CONTACT INFORMATION Dr. 1. Name: Mr. Ms. Mrs. Last First MI 2. Social Security Number: 3.Name and address of organization, agency or any other counseling setting where the applicant gained supervised experience: Name: Address: Street City County State Zip Code 4.
Employment Application
www.bobateacompany.comDate Name Street Address Last First Middle City State Zip Code Day Telephone Evening Telephone Are there other names under which you have worked or attended school? Yes No If yes, please list the name used and location it was used for reference checking purposes. If you are under 18 years of age, do you have a work permit?