Search results with tag "Patient authorization"

580-3271 (6-19) PATIENT AUTHORIZATION FORM
health.mo.govA Patient Authorization Form is required by 19 CSR 30-95.030 as proof of a patient’s desire that a particular individual serve as the patient’s primary caregiver and must be submitted with a Primary Caregiver Registration Application.

FROM: TO - Advocate Health
www.advocatehealth.comWhite - Original in the Medical Record Yellow - Copy to the Patient AUTHORIZATION FOR RELEASE OF PATIENT HEALTH INFORMATION *005013* 00-5013 03/07 Patient Name_____

RHEUMATOLOGY ASSOCIATES Main Phone: 214 …
arthdocs.comRHEUMATOLOGY ASSOCIATES Main Phone: 214-540-0700; Main Fax: 214-540-0701 PATIENT AUTHORIZATION FOR USE AND DISCLOSURE OF PROTECTED HEALTH INFORMATION By signing this authorization, I authorize Rheumatology Associates to use and/or disclose certain protected health information (PHI) about me to Dr. _____

My signature below certifies that I have read, understand ...
www.astellaspharmasupportsolutions.compatient authorization statement My signature on the front of this form authorizes my doctor(s), my healthcare providers, my health plan or payer, and my pharmacy to disclose to Astellas (“Company”) and its third-

PHONE: 844-NEX-4321 (844-639-4321) FAX: 844 …
www.merckcscn.comPatient Authorization (For benefit investigation request only) I understand that in order for Merck Sharp & Dohme B.V., a subsidiary of Merck & Co., Inc., and Lash (the company that will conduct reimbursement services on

Patient Authorization to Disclose, Release and/or Obtain ...
depts.washington.eduPatient Authorization to Disclose, Release or Obtain Protected Health Information. Item #1 (Patient Information): The name, birthdate, phone number and Medical Record Number (if known) of the patient. Item #2 (Purpose): indicate any and all purposes for disclosure.

PATIENT AUTHORIZATION FOR RELEASE OF MEDICAL …
www.mountsinai.orgpatient authorization for release of medical information to third party please print patient information location(s) of service (check only those where you received services): please fill in information and check all boxes that apply
Patient Authorization for Release of Protected Health ...
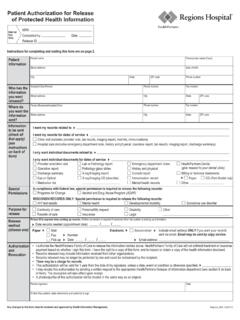
www.healthpartners.comPatient Authorization for Release of Protected Health Information Internal Use Only Completed by Date MRN Release ID City Clinic visit (includes provider note, lab results, imaging report, med list, immunizations) Hospital care (includes emergency department note, history and physical, operative report, lab results, imaging report, discharge ...
Patient Information Sheet (Please fill out - About Us
www.mastormentalhealth.comΨ Jason E. Mastor, M.D., P.A. Kristin C. Brown, PA-C, MMS Please read carefully and sign PATIENT AUTHORIZATION RECORD 1. CONSENT TO TREATMENT: I hereby authorize the physician in charge of my psychiatric care to oversee my

Patient Referral Form n Specialty Pharmacy
www.paragardbvsp.comBenefit Verification SM Benefits Verification SM Specialty Pharmacy SM Patient Authorization Form Specialty Pharmacy SM PARAGARD In accordance with the …