Search results with tag "Marijuana program"
HOW MUCH WILL MEDICAL MARIJUANA COST? Patients
www.health.pa.govMARIJUANA PROGRAM Information for Patients Visit www.medicalmarijuana.pa.gov Pennsylvania Department of Health Office of Medical Marijuana 625 Forster Street Health & Welfare Building Room 628 Harrisburg, PA 17120 717-547-3047 RA-DHMedMarijuana@pa.gov » Pills, oil, topical forms such as patches or ointments.

Adult Use Marijuana Program Licensed Marijuana …
www.azdhs.govAdult Use Marijuana Program Licensed Marijuana Establishments. 3 | Page Updated 06.30.2021 2:00pm Total Licensees: 1 43 . Status Certificate Number Establishment Name DBA Street Address City Zip Code Open . 00000077ESTT45790153 Desertview Wellness & Healing Solutions, LLC Green Pharms 7121 N Hwy 89 Flagstaff 86004 . Open
New York State Medical Marijuana Program
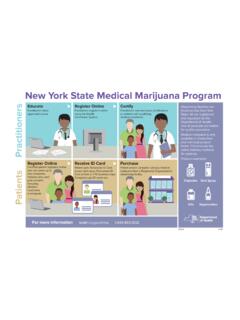
www.health.ny.govMedical marijuana is only available in smoke-free and non-food product forms. This ensures the safest delivery methods for patients. Product examples: Practitioners Patients New York State Medical Marijuana Program Capsules Oral Spray Oils Vaporization #1083 12/18 For more information health.ny.gov/mmp 1-844-863-9312
State Marijuana/Cannabis Taxes - 2022
www.taxadmin.orgJan 06, 2022 · medical-marijuana program, would be responsible for regulating the cultivation, processing, and sale of. recreational marijuana. New York. The legislature has approved and the Governor signed S. 854 which allows for . recreational marijuana sales. beginning April 1, 2022. Taxes: A . tax of 0.5 cent/milligram of THC in Flower

Medical Marijuana Program Qualifying Patient Checklist
azdhs.govMedical Marijuana Program Qualifying Patient Checklist . Please note that this checklist information and other instructions may change. Please refer back to the ADHS website for the most current information. Print out and review this checklist prior to submitting your Qualifying Patient Application in the ADHS online system.

MARIJUANA PROGRAM PATIENT ATTESTATION
azdhs.govMARIJUANA PROGRAM PATIENT ATTESTATION. I, _____ , attest that: I will not divert marijuana to any individual who or entity that is not allowed to possess marijuana pursuant A.R.S. Title 36, Chapter 28.1 and that the information provided in the application is true and correct. _____ _