Example: air traffic controller
ALLERGAN Patient Assistance Program
attached to this application and that all information provided in sections 2.0, 2.1 and 2.3 is correct and complete. I understand that Allergan Pharmaceuticals, Inc. Patient Assistance Program (“Program”) is entitled at any time to request verification of any such information
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

PRODUCT MONOGRAPH INCLUDING PATIENT …
allergan-web-cdn-prod.azureedge.netFIBRISTAL® Ulipristal Acetate, 5 mg tablets Page 1 of 55 PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrFIBRISTAL® ulipristal …

Augmentation
allergan-web-cdn-prod.azureedge.net• Breast implants have been associated with the development of a cancer of the immune system called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL). This cancer occurs more commonly in patients with textured breast implants than smooth implants, although rates are not well defined. Some patients have died from BIA-ALCL.

DIRECTIONS FOR USE FOR THE XEN GLAUCOMA …
allergan-web-cdn-prod.azureedge.net8038-001 Rev E DIRECTIONS FOR USE FOR THE XEN® GLAUCOMA TREATMENT SYSTEM MODEL # 5513-001: XEN® GLAUCOMA TREATMENT SYSTEM DEVICE DESCRIPTION The XEN® Glaucoma Treatment System is comprised of the following sterile components: XEN®45 Gel Stent; preloaded into a XEN® Injector The XEN®45 Gel Stent is a glaucoma implant designed to reduce …

BOTOX® Safety Data Sheet
allergan-web-cdn-prod.azureedge.netSAFETY DATA SHEET Issuing Date 11-Jan-2010 Revision Date 02-Apr-2015 Revision Number 2 1. IDENTIFICATION OF THE SUBSTANCE/PREPARATION AND THE COMPANY/UNDERTAKING GHS product identifier Product Name BOTOX® (Botulinum Toxin Type A) Purified Neurotoxin Complex (50, 100 and 200
Related documents
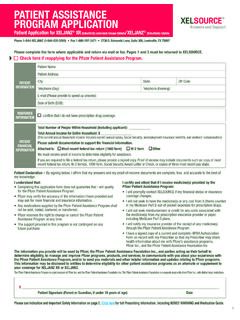
XELSOURCE Patient Assistance Program Application
www.pfizerpro.comThe Pfizer Patient Assistance Program is a joint program of Pfizer Inc. and the Pfizer Patient Assistance Foundation Inc. The Pfizer Patient Assistance Foundation is a separate legal entity from Pfizer Inc., with distinct legal restrictions. Please see Indication and Important Safety Information on page 2.

LILLY CARES FOUNDATION Patient Assistance Program …
www.lillycares.comLILLY CARES® FOUNDATION Patient Assistance Program Application The Lilly Cares Foundation, Inc. (“Lilly Cares”) is a nonprofit organization that offers a patient assistance program (“Program”) to help qualifying patients obtain certain Eli Lilly and Company (“Lilly”) medications at no cost.

GSK Patient Assistance Program Non-Vaccine Application …
www.gskforyou.comGSK Patient Assistance Program Application Check List: Call 1-866-728-4368 with any questions about how to complete this form ddddddd to receive medicines through this program. Please be does not constitute health insurance. Complete all required sections of the application. An incomplete application will delay processing.

Phone: 66-310-7549 MF 8 8 ET Novo Nordisk, Inc. Novo ...
www.novocare.comthe Patient Assistance Program) express consent to receive automated and prerecorded phone calls from Novo Nordisk and its Patient Assistance Program partners on the phone number provided on your Patient Assistance Program application. You also understand that you will be asked to provide your social security number and date of birth
Viatris Patient Assistance Program (PAP) Application
www.viatris.comThe PAP Application must be complete to be reviewed for patient program eligibility. Please ensure all areas of the form are completed in full, including all signatures. To be considered for the Viatris Patient Assistance Program, all applicants must satisfy the following requirements and eligibility criteria:

Patient Assistance Program Application - JJPAF
jjpaf.orgPatient Assistance Program Application. INSTRUCTIONS FOR ENROLLMENT. Ask your Healthcare Professional (HCP) to complete, and . sign and date. page 3. Submit completed pages . 2 and 3 only. with documentation to: Mail: Johnson & Johnson Patient Assistance Foundation, Inc. Patient Assistance Program. PO Box 0367, Chesterfield, MO 63006. Fax:

Patient Assistance Program PO BOX 66764, St. Louis, MO …
www.allergan.comPatient Assistance Program at (844) 424-6727 for instructions. Fax or mail the completed application and documentation to: • Allergan Patient Assistance Program PO BOX 66764, St. Louis, MO 63166 Phone: 1 844-424-6727 Fax: 1 844-708-0036 • Upon receipt of a completed application, notification of eligibility will be sent to the

Pfizer Patient Assistance Program
www.pfizerencompassresources.comThe Pfizer Patient Assistance Program is a joint program of Pfizer Inc. and the Pfizer Patient Assistance Foundation. The Pfizer Patient Assistance Foundation is a separate legal entity from Pfizer Inc., with distinct legal restrictions. P.O. Box 220040, Charlotte, NC 2222 T: …