Example: barber
Authorization for Use or Disclosure of Medical Information
this Authorization will need my further written authorization to re-disclose this information. 42 CFR §2.32 restricts any use of this information to criminally investigate or prosecute any alcohol or …
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

The prescribing physician must sign and clearly printname ...
www.optimahealth.com1 . OPTIMA HEALTH PLAN. PHARMACY PRIOR AUTHORIZATION/STEP-EDIT REQUEST* Directions: The prescribing physician must sign and clearly print. name (preprinted stamps not valid) on this request.

2018 Optima Vantage Plans
www.optimahealth.comOptima health is the trade name of Optima Health Plan, Optima Health Insurance Company, Optima Health Group, Inc. and Sentara Health Plans, Inc. Optima Vantage HMO and POS plans are underwritten by Optima Health Plan.

Claim Payment Reconsiderations - Optima Health
www.optimahealth.comPROVIDER MANUAL A SERVICE OF SENTARA A PUBLICATION OF THE OPTIMA HEALTH NETWORK MANAGEMENT DEPARTMENT This version of the Optima Health Provider Manual was last ...

2019 STANDARD ALTERNATIVE DRUG LIST (January - …
www.optimahealth.com1 2019 STANDARD ALTERNATIVE DRUG LIST (January - March 2019) Product Label

Maximum Allowable Daily Dosage and ... - Optima Health
www.optimahealth.combupropion tab 100mg er 4.5 tabs/day bupropion tab 100mg sr 4.5 tabs/day bupropion tab 150mg . two 90 day supplies/183 days bupropion tab 150mg er 3 tabs/day

2019 STANDARD ALTERNATIVE DRUG LIST (July - …
www.optimahealth.comThe alternatives listed are suggestions based on how the drug works and the condition it treats. You should discuss your therapy with you doctor or health care provider.
Related documents
DOC-1163A Authorization for Use and Disclosure of ...
doc.wi.govspecific protected health information authorized for use/ disclosure this authorization applies to medical, mental health, developmental disability and alcohol/drug abuse information, and hiv test results, unless excluded below. i do not want the following information disclosed.
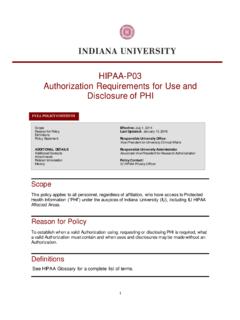
HIPAA-P03 Authorization Requirements for Use and ...
compliance.iu.eduAuthorization to use or disclose PHI for a research study may be combined with other types of written permission for the same research study provided the conditions for a valid Authorization are satisfied.
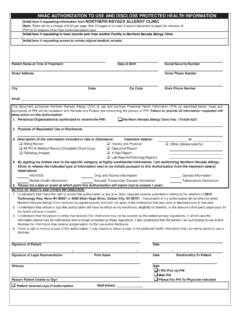
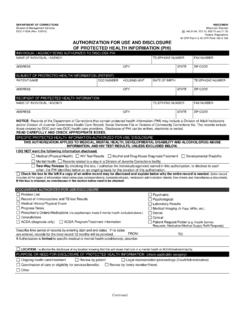
NNAC AUTHORIZATION TO USE AND DISCLOSE PROTECTED …
www.nevallergy.comAUTHORIZATION TO USE AND DISCLOSE PROTECTED HEALTH INFORMATION (PHI) IMPORTANT INFORMATION » The Authorization To Use And Disclose Protected Health Information form must be filled out in its entirety. Failure to properly complete the form will result in …

LOS ANGELES COUNTY DEPARTMENT OF MENTAL HEALTH ...
lacdmh.lacounty.govlos angeles county department of mental health authorization for use or disclosure of protected health information mh 602 (09/2016) page 1 of 2

Authorization for UW Medicine to Use or Disclose Protected ...
depts.washington.eduauthorization, except in these cases: (1) UW Medicine may condition researchrelated treatment on - my signing or my providing an authorization for the use or disclosure of my information for such research or (2) UW
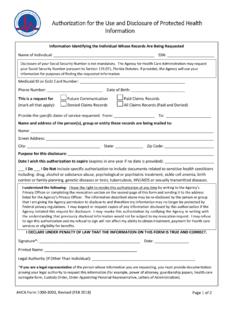
Authorization for the Use and Disclosure of Protected ...
www.ahca.myflorida.comAuthorization for the Use and Disclosure of Protected Health Information . Page 2 of 2 . Instructions for Completing the Authorization for the Use and Disclosure of Protected Health Information Form. 1. Complete the first page of this form and return it to:
Authorization for Use or Disclosure of Health Information
www.cmhshealth.orgThis authorization expires (insert date): _____ This authorization expires one (1) year from date signed below unless a specified date is documented above. After you have filled out this form, please print it and bring it to Medical Records at CMH to complete the request process.
AUTHORIZATION to Use or Disclose Protected Health ...
ufhealthjax.orgAUTHORIZATION to Use or Disclose Protected Health Information (PHI) - General Purposes Patient Name Verification of Identity (Driver’s License, ID Card, Passport, etc.) Address Health Record Number Phone # Phone # E-mail Address Date of Birth
Authorization for Use & Disclosure of Information
www.dhs.state.or.usDHS 2099 (8/04) Page 1 of 2 Authorization for Use & Disclosure of Information This form is available in alternative formats including Braille, computer disk, and oral presentation.
Authorization to Use and Disclose Health Information
accredo.comAuthorization to Use and Disclose Health Information . I authorize . Accredo Health Group. to use or disclose my health information as described below. I understand that the information I authorize a person or entity to disclose may be shared with other people