Example: dental hygienist
Authorization to use and disclose health information
Authorization to use and disclose health information (Request copies of medical records) Health Information Management For Cape Canaveral Hospital, Holmes Regional Medical Center, Palm Bay Hospital, Viera Hospital, and their affiliates.
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

Medical Prior Authorization List - Health First
hf.orgPage 4 of 88 75572 Computed tomography, heart, with contrast material, for evaluation of cardiact structure and morphology (including 3D image postprocessing, assessment of cardiac function, and

January 1 – December 31, 2019 Evidence ofCoverage
hf.orgbetween January 1, 2019 and December 31, 2019. Each calendar year, Medicare allows us to make changes to the plans that we offer. This means we can change the costs and benefits of the SunSaver Plan (HMO) after December 31, 2019. We

The following codes are authorized by Palladian Health for ...
hf.orgCode Code Description 20974 Electrical stimulation to aid bone healing; noninvasive (nonoperative) 20975 Electrical stimulation to aid bone healing; invasive (operative)

Billing Guideline Subject: Preventive Services Background
hf.orgPreventive care and screenings for women, infants, children, and adolescents that are provided ... Contraceptive Services and Supplies Contraception 36 - 38 . Billing Guideline for Preventive Services P a g e | 1 Revisions from last publication are highlighted in yellow.

How to Set Up Microsoft Authenticator
hf.orgA. Get the Authenticator app 1. On your iPhone, open your Apple App Store - or on your Android phone, open your Google Play Store . 2. Search for, download and install the Microsoft Authenticator app . (There is no cost for this app.) B. Set up the app 1. On your separate device, visit MyAccount.Microsoft.com. 2.
Related documents
DOC-1163A Authorization for Use and Disclosure of ...
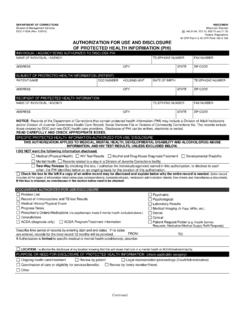
doc.wi.govspecific protected health information authorized for use/ disclosure this authorization applies to medical, mental health, developmental disability and alcohol/drug abuse information, and hiv test results, unless excluded below. i do not want the following information disclosed.
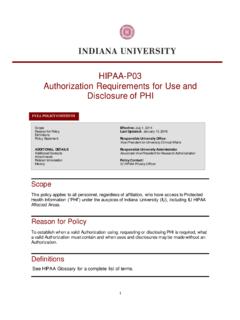
HIPAA-P03 Authorization Requirements for Use and ...
compliance.iu.eduAuthorization to use or disclose PHI for a research study may be combined with other types of written permission for the same research study provided the conditions for a valid Authorization are satisfied.
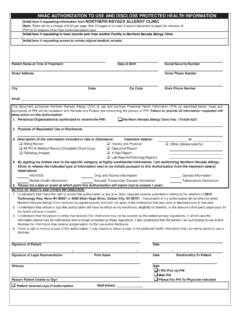
NNAC AUTHORIZATION TO USE AND DISCLOSE PROTECTED …
www.nevallergy.comAUTHORIZATION TO USE AND DISCLOSE PROTECTED HEALTH INFORMATION (PHI) IMPORTANT INFORMATION » The Authorization To Use And Disclose Protected Health Information form must be filled out in its entirety. Failure to properly complete the form will result in …

LOS ANGELES COUNTY DEPARTMENT OF MENTAL HEALTH ...
lacdmh.lacounty.govlos angeles county department of mental health authorization for use or disclosure of protected health information mh 602 (09/2016) page 1 of 2

Authorization for UW Medicine to Use or Disclose Protected ...
depts.washington.eduauthorization, except in these cases: (1) UW Medicine may condition researchrelated treatment on - my signing or my providing an authorization for the use or disclosure of my information for such research or (2) UW
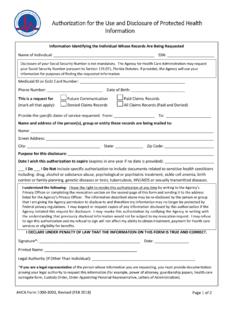
Authorization for the Use and Disclosure of Protected ...
www.ahca.myflorida.comAuthorization for the Use and Disclosure of Protected Health Information . Page 2 of 2 . Instructions for Completing the Authorization for the Use and Disclosure of Protected Health Information Form. 1. Complete the first page of this form and return it to:
Authorization for Use or Disclosure of Health Information
www.cmhshealth.orgThis authorization expires (insert date): _____ This authorization expires one (1) year from date signed below unless a specified date is documented above. After you have filled out this form, please print it and bring it to Medical Records at CMH to complete the request process.
AUTHORIZATION to Use or Disclose Protected Health ...
ufhealthjax.orgAUTHORIZATION to Use or Disclose Protected Health Information (PHI) - General Purposes Patient Name Verification of Identity (Driver’s License, ID Card, Passport, etc.) Address Health Record Number Phone # Phone # E-mail Address Date of Birth
Authorization for Use & Disclosure of Information
www.dhs.state.or.usDHS 2099 (8/04) Page 1 of 2 Authorization for Use & Disclosure of Information This form is available in alternative formats including Braille, computer disk, and oral presentation.
Authorization to Use and Disclose Health Information
accredo.comAuthorization to Use and Disclose Health Information . I authorize . Accredo Health Group. to use or disclose my health information as described below. I understand that the information I authorize a person or entity to disclose may be shared with other people