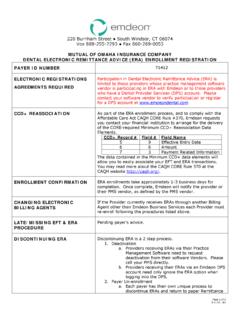
Transcription of Change Healthcare ERA Provider Information Form - Emdeon
1 PAYER ID: 60054 SUBMITTER ID: Change Healthcare ERA Provider Information form *This form is to ensure accuracy in updating the appropriate account 1 Provider Organization Practice/ Provider Name Facility Name Tax ID Client ID Site ID. Address City STATE ZIP. Contact Name E-mail Address Telephone Fax 2 Vendor ( Change Healthcare certified vendor used to submit files to Change Healthcare ). Vendor Name Vendor Submitter ID. Contact Name E-mail Address 3 Payer Payer ID 60054 AETNA. Group ID Individual Provider ID NPI ID.
2 4 Confirmations Send Change Healthcare Claim Confirmations To: Special Instructions: All Payer Registration forms must contain signatures when applicable, stamped signatures or photo copies are accepted. SUBMIT COMPLETED form TO: Fax: (615)231-4843. Email: PROVIDERS MUST BE SENDING ELECTRONIC CLAIMS TO RECEIVE ELECTONIC REMITTANCE. THE FOLLOIWNG form MUST BE PROCESSED BY Change Healthcare . DO NOT SEND TO THE PAYER. SOLO. PRACTIONERS WITH NO OFFICE MANAGER PLEASE SIGH IN BOTH BOXES "EFT IS REQUIRED. PLEASE NOTE.
3 "ALREADY ON FILE" IF EFT IS SETUP. Change Healthcare REVISION form DATE: 05/11/16. Change Healthcare ENROLLMENT HELP DESK. 866 924-4634