Transcription of Consequences of Alcohol Use in Diabetics
1 Vol. 22, No. 3, 1998211 Consequences of Alcohol Usein DiabeticsNicholas V. Emanuele, , Terrence F. Swade, , and Mary Ann Emanuele, hormone insulin, which is produced in the pancreas, is an important regulator of blood sugarlevels. In people with diabetes, the pancreas does not produce sufficient insulin (type 1 diabetes)or the body does not respond appropriately to the insulin (type 2 diabetes). Alcohol consumptionby Diabetics can worsen blood sugar control in those patients. For example, long-term Alcohol usein well-nourished Diabetics can result in excessive blood sugar levels. Conversely, long-term alco-hol ingestion in Diabetics who are not adequately nourished can lead to dangerously low bloodsugar levels. Heavy drinking, particularly in Diabetics , also can cause the accumulation of certainacids in the blood that may result in severe health Consequences . Finally, Alcohol consumptioncan worsen diabetes-related medical complications, such as disturbances in fat metabolism, nervedamage, and eye disease.
2 KEY WORDS: AODE ( Alcohol and other drug effects); diabetes; glucose;insulin; pancreas; heavy AOD use; adverse drug effect; disease complication; nutrient intake;ethanol metabolism; hypoglycemia; ketoacidosis; lipid metabolism; triglycerides; cholesterol; patho-logic process; cardiovascular disorder; neuropathy; psychosexual dysfunction; visual systemdisorder; literature reviewiabetes mellitus, which affectsan estimated 16 million peoplein the United States, is a com-plex disorder interfering with the body ssugar ( , carbohydrate), fat ( , lipid),and protein metabolism. The disease iscaused in most cases by a deficiency orcomplete lack of the hormone insulin,which is produced in the pancreas, orby an inability of the body to respondappropriately to insulin ( , insulinresistance). The results of both condi-tions can include chronically elevatedblood sugar levels, excessive excretionof sugar in the urine, and the accumu-lation of certain acidic substances inthe blood.
3 If not prevented or treatedproperly, these changes can lead tocoma and even death. Other adverseevents associated with diabetes affectthe eyes, kidneys, nervous system, skin,and circulatory system. Because Alcohol use, at least on asocial level, is widespread among diabet-ics as well as nondiabetics, clinicians andresearchers must understand Alcohol seffect on the progression and compli-cations of diabetes. This article firstreviews the pathophysiology of the twomajor forms of diabetes, type 1 and type2. It then summarizes the current stateof knowledge regarding Alcohol s effectson blood sugar regulation and otheraspects of metabolism as well as on thecardiovascular, neurological, and eye com-plications associated with the disease. Pathophysiology ofDiabetes MellitusThe two most common forms of dia-betes are type 1 and type 2 diabetes,with type 2 diabetes accounting for atNICHOLASV. EMANUELE, , is aprofessor in the Department of Medicine,the Division of Research on Drugs of Abuse,and the Molecular Biology Program anddirector of the Division of Endocrinologyand Metabolism at Loyola UniversityStritch School of Medicine, Maywood,Illinois, and a staff physician at the VeteransAffairs Hospital, Hines, SWADE, , is in the private practice of endocrinology in theChicago, Illinois, , , is a professor in the Department of Medicine,the Department of Molecular andCellular Biochemistry, and the Divisionof Research on Drugs of Abuse, LoyolaUniversity Stritch School of Medicine,Maywood, Health & Research Worldleast 90 percent of all cases.
4 Type 1diabetes is an autoimmune disease that is, a disease in which the body simmune system attacks and destroysnot only foreign molecules or organ-isms but also some of the body s owncells. In most patients, the diseasedevelops before age 40, primarily dur-ing childhood or adolescence. Inthose patients, the immune systemattacks certain cells of the pancreas,called beta cells. (For more informa-tion on the structure and function ofthe pancreas, see textbox, p. 213.)Beta cells produce insulin, one of thetwo major hormones involved in reg-ulating the body s blood sugar levelsand other metabolic functions. Mostimportantly, insulin leads to the uptakeof the sugar glucose into muscle andfat tissue and prevents glucose releasefrom the liver, thereby lowering bloodsugar levels ( , after a meal) (see fig-ure). As a result of the immune system sattack, the beta cells can no longer pro-duce insulin.
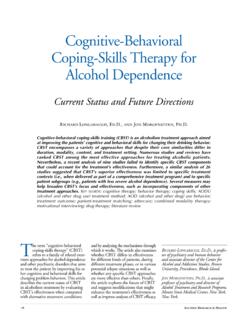
5 Consequently, the patientessentially experiences total insulinlack. Because insulin is a key metabolichormone, insulin deficiencyleads tomajor impairment of the body s regula-tion of carbohydrate, lipid, and pro-tein metabolism. Type 2 diabetes, which in mostcases develops in people over age 40,has a somewhat different pathophys-iology than type 1. People with type2 continue to produce insulin inearly disease stages; however, theirbodies do not respond adequately tothe hormone ( , the patients areresistant to insulin s effects).Thus,insulin does not lower blood sugarlevels to the extent that it does inpeople without diabetes. The insulinresistance is partly inherited andpartly acquired. For example,obesity, inactivity, and cigarettesmoking may worsen geneticallydetermined insulin resistance. Insulin resistance does not immed-iately lead to overt diabetes, because thepatient s pancreatic beta cells initiallycan increase their insulin productionenough to compensate for the insulinBlood glucose regulation by insulin in healthy people and in people with type 1 or type 2 cellsNormal insulin productionNormal pancreasFood intakeBlood glucose levels increasefollowing food digestion andabsorption in the gastrointestinal or very little insulin productionType 1 diabetesType 2 diabetesNormal or even elevated insulin production Blood glucose is taken up into muscle and fat tissue and used in metabolic processes.
6 No additional glucose is generated in the liver, and existing glucose is converted into a storage form ( , glycogen) as a reserve in case blood glucose levels drop too low. Blood glucose levels returnto their normal range. Blood glucose levels remain high, eventually leading to serious complications. Both protein and fat metabolism are impaired, eventually leading to serious complications. The body resists insulin s effects. Initially, resistance can be overcome by increasing insulin production. Eventually, the body can no longer produce enough insulin; the same complications occur as with type 1 of Alcohol Use in DiabeticsVol. 22, No. 3, 1998213resistance. In fact, insulin-resistantpeople have higher than normal insulinlevels ( , are hyperinsulinemic1). Intime ( , probably after several years),however, the pancreas cannot keep upwith the increased demand for insulin;although insulin production still maybe higher than in nondiabetic people, itis no longer sufficient to overcomeinsulin resistance.
7 Ultimately, insulinsecretion declines even further, to levelsbelow those seen in nondiabetics(although generally still higher thanthose seen in type 1 Diabetics ). At thatpoint, when a deficit in insulin secretionis combined with a state of insulinresistance, the person develops type 2diabetes. Thus, whereas type 1 diabetesis characterized by a complete lack ofinsulin production, type 2 is charac-terized by reduced insulin productionplus insulin resistance. The reasonsunderlying defective insulin secretionand insulin resistance, which are stillunder investigation, are complex andbeyond the scope of this article (for areview, see DeFronzo 1997).People with either type 1 or type 2diabetes generally are treated withinsulin injections or for people withtype 2 with medications that stimu-late the body s own insulin production( , a class of medications called sulfonylureas or an agent calledrepaglinide).
8 Those medications, how-ever, may lead to lower than normalblood sugar levels ( , hypoglycemia):As the medications enhance insulinproduction, the body responds to theincreased insulin levels by increasingglucose uptake into the muscle andfat tissue and decreasing glucose secre-tion from the liver. As a result, thebody s hormone system mounts acounter-regulatory response: It secretesan array of hormones that throughvarious mechanisms raise blood sugarlevels back to normal. The mostimportant of those counter-regulatoryhormones are glucagon, which is pro-duced in pancreatic alpha cells, andepinephrine, which is secreted fromthe adrenal glands. Other hormonesinvolved in the counter-regulatoryresponse include growth hormone,which is produced in the pituitarygland, and cortisol, which is producedin the adrenal glands. (For moreinformation on those hormones andtheir functions, see the article by Hiller-Sturmh fel and Bartke, pp.)
9 153 164.)With increasing duration of diabetes,however, the counter-regulatoryresponses of first glucagon and thenepinephrine wane, rendering the dia-betic patient more vulnerable tosevere hypoglycemia, whether it resultsfrom medications or other causes. Two additional medications met-formin and troglitazone are now beingused to treat people with type 2 agents act to lower the patient sblood sugar levels by decreasing insulinresistance rather than by increasinginsulin secretion. Accordingly, thesemedications help control blood sugarlevels without causing s Effects on Blood Sugar Levels of DiabeticsNumerous studies have investigatedalcohol s effects on the control ofblood sugar levels in Diabetics . Thoseeffects differ substantially dependingon whether Alcohol consumptionoccurs when the person has just eatenand blood sugar levels are relativelyhigh ( , in the fed state) or whenthe person has not eaten for severalhours and blood sugar levels are rela-tively low ( , in the fasting state).
10 Effects of Alcohol Consumption in the Fed StateIn people with either type 1 or type 2diabetes, single episodes of alcoholconsumption ( , acute Alcohol con-sumption) generally do not lead toclinically significant changes in bloodsugar levels. In fact, some studies haveindicated that isolated episodes ofdrinking with a meal may have a ben-eficial effect by slightly loweringblood sugar levels that tend to rise toohigh in Diabetics (Swade and EmanueleThe Pancreas and Its HormonesThe pancreas, which is located behind the stomach, serves two functions. Thefirst function, which involves most of the pancreatic cells, is the productionof digestive enzymes. Those enzymes are secreted directly into the gut toensure effective food digestion. The second function is the production ofseveral hormones. Two of the hormones ( , insulin and glucagon) arepotent regulators of blood sugar levels. Both hormones are produced in areasof the pancreas called the Islets of Langerhans, which, quite literally, are islands of hormone-producing cells in a sea of digestive enzyme-producingcells.)