Transcription of Contracted Provider Information Change/Update …
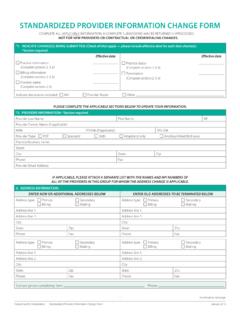
1 G:\providersvcs\pif and wpa folder\ Contracted Provider change Provider change 1 Contracted Provider Information Change/Update form This form is f or Contracted Kaiser Permanente providers to notify us of any new Information or changes to their current practice structure. Complete form (s) can be emailed to The fields marked with an asterisk (*) under this section are required for all changes/updates. Contracted Provider Information *Contact Name:*Contact Phone:*Contact E-mail:*Contact Tax ID:*Type of Change/Update Address (any type) New Clinic Name Phone Number (any type) Fax Number (any type) Add New Location Tax ID changes (please include new W-9) *Effective Date of change :Please describe the changes you are making. Comments: Enter your current Information under this section.
2 Only complete the fields where the current Information Kaiser Permanente has on file is changing. Clinic/Service Location Address Current/Old Information : New/Updated Information : Clinic/ Provider Name: Address: City State Zip Phone Fax Website address Office Contact e-mail Contracted Provider Information Change/Update form 2 Remit/ Pay To Address If enrolled in Electronic Funds Transfer you must also notify InstaMed of Billing NPI and Tax ID changes by emailing or Contact InstaMed Customer Service toll-free at 1-877-833-6821 Current/Old Information : New/Updated Information : Remit/Pay To Name Address: Street Address: City State Zip Phone Pay To NPI Tax ID change /Tax ID Address change /1099 IRS Reporting Address change /Contract Notification Address change (I nclude an updated W9) Current/Old Information : New/Updated Information .
3 Tax ID number Tax ID Address: Street Address: City State Zip Phone Pay To NPI Please email the completed form to Provider Services at This form is not for adding practitioners. If you are adding a new practitioner please send an email requesting the :\providersvcs\pif and wpa folder\ Contracted Provider change Provider change