Transcription of CORTICOSTEROID INDUCED AVASCULAR …
1 CHAPTER 35 INTRODUCTIONAva scu lar nec ro si s (AVN) is a pr oc ess that is du e to thete mp ora ry o r p er manent loss o f th e bloo d sup pl y to anarea of b on e. As a resul t, the bone ti ssue di es a nd the bonecol la ps es . If t he AV N involves a j oint , it can lead to destru ction of cartilage, re sulting in arth ritis and N c an be classi fi ed into 2 g ene ral c ategor ies , trau mati c and non traum ati c. I n the case of trau ma , a fract uredis rupts the blood supply to the bone leadi ng t o AVN. In the ca se of nont raumatic AVN, some ot her path ol ogy dis rupts the blood vessels. Thes e i nc lude idiopat hi c (n o ca use is ev er f ound), steroi ds ( ., anabolic a nd h igh dose- cor tic oste roids [pred nis one ] g ive n for rheuma toidar thr it is, lupus, or cancer), excess al cohol consumpt ion ,sic kl e ce ll an emia, or rad iatio n t reat ments (1 ).
2 The cas e pr esen tation is a pat ien t with chronic pain atthe fir st me tat ars al-m edial cunei form joi nt and medi alcu nei form bone , t reat ed with multiple cort ico st eroid inj ecti ons . T he patient devel op ed AVN of the m edi alcu nei form bone with subsequent arthrit is of t he fi rstmet ata rsome di al c uneif orm and medial cune if orm-navicu larjoi nts. The diagnosis was made by phy sica l e xa mi nat ion,pl ai n rad iog ra ph s, an d magneti c r esonan ce imaging ( MRI) .The s ym ptoms were alleviated wit h a rthr odesis of t hesejo int s u sing ext ern al f ix ati on, and he mo po ieti c autol ogo usbon e g raft co mb ined wi th al logenous bone graft. CASE REPORTA 62-year- old ma n presented wi th a repo rt o f a d ul l, achin gpa in in t he medi al aspect of hi s ri ght m id foo t an d ri ght fi rstray o f 1 y ear o f d ura tion. T he p ain w as no ted to in creaseafter str enuous walking, and when h e wears any ty pe of e pati ent st ate d that the pain was persi st ent and ranke d10 out of 10 on a pain scale.
3 There was asso ciat ed swellin gobserve d in the r ig ht fo ot. Th e pat ient repo rted rec eivin g mu lt ipl e cort ic ostero id i nj ect ions in th e r ig ht m edialcune iform area by di ff eren t do ctors du e to t he chroni c pai was no other pas t medic al his tor y tha t would inc re aseth e li ke lih ood of b one i nf arct io n, such as rh eumat oi d art hritis , lu pu s, can cer, ex ces s a lco hol cons umption, sic klecel l a nemia , or ra di at io n t rea tm ent s (1) .An ta lg ic g ai t wa s n ot ed on gross exam inati on , mi ldsw el lin g a nd pa in on pa lpa tio n were note d ove r t he me dialcune iform are a wit h pain fu l a nd li mi ted range of mo ti on ofthe right fir st ray. Moti on of the right a nkle and subtala r joi ntwere nor ma l. P re ope ra tiv e ra di og ra phs (Fi gure 1) and MRIof the ri ght f oot w ith a nd w it hout c ontrast (Figure 2) wer eobta ined.
4 Th e pa tie nt ha d b ee n tre ated by dif fer ent docto rswi th lim ited wei ght bea ri ng on th e r igh t lo wer ex tremity andcort icost ero id i nj ect io ns. T he pati ent c ont inu ed t o have se vere p ain t o his ri gh t mi dfo ot aft er wei gh tb ear in g re stri ctions a nd ste roi d i nj ection s f or a bo ut 1 year. Based onth e c lin ica l eva luatio n and diag no stic ima ge findings , AVN ofthe ri ght me dia l cu ne iform w as di ag nose ev ac uat io n an d cur ett ag e of the cun eifo rm wasplan ne d w ith art hr odesis of t he fi rst met at arsal -med ialcun ei form and me dial cun eif orm- nav icul ar bone joints . Bonegraft ap plica ti on was T rinit y Ev ol ution bo ne al log raft com bi ne d wit h he mop oi eti c au to logous b one g raft . Thearth rode sis was pl anne d to b e pe rf orm ed usi ng 2 mini -railex ter na l f ix ators f rom Ortho fi x.
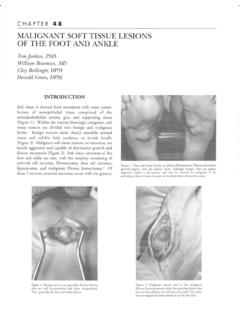
5 Al l be nefit s and ri sks abo ut the pr oced ure were disc usse d with the pa ti ent and the p atie nt gav e conse nt fo rthe su rg ic al pr oc edu te r a nest hesi a wa s o bta ine d, a n i nc isi on was madeover th e rig ht fir st meta ta rs al- med ia l c une iform joint andex te nde d to the ri ght me dia l c une if or m-nav icul ar joi ing m ild d ist ract ion at t he level of t he medialcun ei fo rm- firs t me tat arsal j oint, t he cart il age from theba se o f th e fi rst m etat ar sal b as e an d from the d ista l as pe ct of the me dial c uneif orm were r emove d in total. I twa s n ote d tha t the med ia l cune if or m had an appearan ceCORTICOSTEROID INDUCED AVASCULAR NECR OSIS OF THE RIG HT MEDIAL CUNEIFORM TREAT ED WITHTR INI TY EVOLUTION BONE GR AF T AND ARTHRODESIS:Case Report an d Rev iew of t he LiteratureThomas J. Merrill, DPMR iquel Gonzalez, DPM CHAPTER 35197 Figure 1D.
6 Lateral view. Figure 1A. Plain radiographs of the right,anterior posterior view revealed the presenceof diffuse sclerosis areas with a possiblenondisplaced subcortical fracture along thedistal margin of the medial cuneiform, andnarrowing of the first metatarsal medialcuneiform joint with diffuse arthriticchanges at the midfoot 1B. Medial oblique view. Figure 1C. Lateral oblique view. CHAPTER 35198 Figure 2C. Sagittal T2 image after contrast material injection. Figure 2A. Preoperative axial T2 magnetic resonance image of the right foot revealed the presence of moderate marrow edema within the medial cuneiform emanating from a probable non-displaced sub-cortical fracture along the distalmargin. Additional mild marrow edema in the proximal and lateral margin of the first metatarsalbase, which may represent an additional stress reaction or contusion, if there has been recenttrauma. The nearby Lisfranc ligament is 2B. Preoperative aixal T2 images aftercontrast material with fat saturation sequences.
7 Figure 2D. Axial T2 images after contrast materialinjection. CHAPTER 35199of ost eop orotic bo ne and had a l ow vascu lar natu en at tent ion was dire cted to t he r igh t navicu lar-media l cunei form joint, wh ere al l t he c arti lage from thejo int sur face were removed in tota l u sin g d ist ract iontech niq ues. T he art icular surfac es of t he jo int s were part ia lly e burnated, and a ll the articul ar surf aces wer edrill ed to obtain good bone bleed in g. Th e j oi nt sp ace swe re f illed with Trinity Evoluti on bon e allograft co mb ine d wi th he mopoietic aut olo gous bone graft andth e art hr od es is was performed using 2 m ini-rail ex ter nalfix ato rs fr om O rt hof ix (Figure 3). Th e surgic al woundwas c lo sed i n an at omic l ayer s an d a s ter il e dressi ng app lie d. T he pa tie nt w as di sc ha rg ed to hi s home wi thver bal an d wri tten i nst ruct ion s rega rd ing n on -wei ghtbeari ng to th e ri ght fo ot an d pa in m edicat ions to beta ke n un til the ne xt posto pe ra tive a ppoi ntme nt.
8 Subse que nt hist opa th olog ic an al ysi s re vealed fragme ntsof ne cro ti c bo ne and bone wit h deg en erati ve oste oar thriti cch ang es con sis te nt w it h th e di ag no sis o f A VN and os te oar thr iti s. The p atient s midf oot pain subsided al mostimm edi at el y aft er the op erat ion, wi th t he exception of su rgic al w ou nd pa in, w hic h sub side d in a n or mal f ash ion. Figure 3A. Intra-operative anterior posterior viewof arthrodesis of the first metatarsal-medialcuneiform and medial cuneiform-navicular bonejoints with application of Trinity Evolution boneallograft combined with hemopoietic autologousbone graft using 2 mini-rail external fixators fromOrthofix 3B. Lateral view. Figure 4B. Postoperative view. Figure 4A. Lateral radiograph of the right foot was taken as part of the postoperative evaluation showing good position of the 2 mini-rails externalfixators and good alignment of the arthrodesis of the first metatarsal-medialcuneiform and medial cuneiform-navicular bone 35200 One we ek following sut ure removal, t he patient wasmobi li zed with pa rtial weightbea ri ng fo r 3 weeks , follo we dby weigh tb ear ing as tolerated fo r the n ext few pos toperat iv ewee ks.
9 Cli nic al a nd radiologic exam inations we re done onthe fir st postopera tiv e day (Figure 4), at 6 we eks, at 9 w eek s,and eve ry other m onth thereafter , unt il ra di ol ogi c conf irmati on o f graft consolidatio n. E xtern al fi xa tio n w as removed 9 w eeks after surgery . Rad iogra ph s sh owed that therigh t fi rst metatarsa l-med ial cunei fo rm and navic ular-me dialcuneiform join ts w ere fu lly f used (Figu re 5 ).DISCUSIONAsi de fro m inj ur y, one of the most com mon c auses of oste on ec rosis i s the use of corti coste roid me dicatio ns su ch aspredn iso ne. Corti costeroids are commonly use d to tr ea t infl am mato ry di se ases such as lupus, rheumatoi d a rthr itis, in -fla mmat or y bowe l disease, severe asthma, and va scu li ud ies s ug ges t tha t long- term us e of or al or in trav en ous cor -ticost eroi ds is associat ed with nont rau mati c osteo ne cros is (2).
10 Isol ated steroi d injection INDUCED oste onecr osis o f the medial c une ifo rm b one is ext rem ely rare . Resea rc hers are notsu re wh y t he use of corticoste roi ds some tim es l eads to oste on ec rosis. They spe culat e t hat t he drugs may i nte rfer ewith the body s a bi lity to break do wn fa tty su bsta nces cal ledlipi ds. Th ese substances the n build up in a nd c log t he b loo dves sels, cau sing them to narrow an d to reduce the amount ofblo od th at ge ts t o the bone. Some studie s s uggest that corti co st eroid -re lat ed o st eo ne crosis i s mor e severe tha n ost eon ec ro sis r es ulti ng fr om o th er ca uses (3-5 ). Th ere a re sev eral p at ho physi ol og ic al cau ses f or the is che mia th at ha ve been postu la te d as th e et iol og ical bas is fo r AVN. One in vo lv es an acc el erat io n of the b on edegrad ati on versu s sy nthesi s.