Example: tourism industry
Customer Appeal Request - Cigna
Customer Appeal Request. An appeal is a request to change a previous adverse decision made by Cigna. You or your representative (Including a physician on your behalf) may appeal the adverse decision related to your coverage.
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

Multi-language Interpreter Services - cigna.com
www.cigna.com[Portuguese] ATENÇÃO: Tem ao seu dispor serviços de assistência linguística, totalmente gratuitos. Para clientes Cigna atuais, ligue para o número que se encontra no verso do seu cartão de identificação.
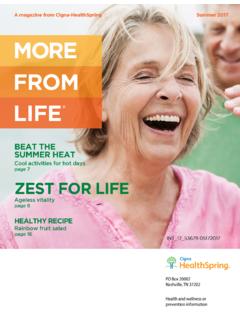
More From Life Summer 2017 - Cigna Health …
www.cigna.comMORE FROM LIFE ® A magazine from Cigna-HealthSpring Summer 2017 PO Box 20002 Nashville, TN 37202 Health and wellness or …
Group - Assocation Proof of Loss Life Insurance …
www.cigna.comi. INSTRUCTIONS FOR FILING A CLAIM SECTION A: EMPLOYEE INFORMATION. Name of Employee/Member (Last Name) (First Name) (Middle Initial)
Atypical Antipsychotics Coverage Determination …
www.cigna.comAtypical Antipsychotics Coverage Determination (FOR PROVIDER USE ONLY) Dosage Frequency Quantity Other Questions: For Aripiprazole and Rexulti:

Cigna Group Universal Life and Group Variable …
www.cigna.com568796 Rev. 03/2017 ® ® ® ® If your life insurance benefit is less than $5,000, Cigna will send you a check for the total benefit amount. Cigna Group Universal Life and

IN-HOME DELIVERY AND HOME HEALTH SERVICES
www.cigna.comHome delivery of medical equipment and supplies (continued) Compression garments Compression (tight-fitting) clothing for all areas body used to help post-surgery healing and improve circulation.

ANNUAL NOTICE OF CHANGES FOR 2017 - Cigna
www.cigna.comCigna-HealthSpring Rx Secure (PDP) Annual Notice of Changes for 2017. Drug Tier 1: Drug Tier 4: 3 . Summary of Important Costs for 2017 . The table below compares the 2016 costs and 2017 costs for Cigna-HealthSpring Rx …

ANNUAL NOTICE OF CHANGES FOR 2017 - Cigna
www.cigna.comCigna-HealthSpring Rx Secure (PDP) Annual Notice of Changes for 2017 2 . Think about Your Medicare Coverage for Next Year . Each fall, Medicare allows you to change your Medicare health and drug coverage during the Annual Enrollment Period.

MAJOR NEUROCOGNITIVE DISORDER (MND): …
www.cigna.comApraxia Agnosia confusion Provider’s guide to diagnose and code Non-Reversible MND MAJOR NEUROCOGNITIVE DISORDER (MND): NON-REVERSIblE FORM
CIGNA DENTAL CARE® (*DHMO) PATIENT CHARGE …
www.cigna.com• This Patient Charge Schedule applies only when covered dental services are performed by your Network Dentist, unless otherwise authorized by Cigna Dental
Related documents

Practitioner and Provider Compliant and Appeal Request
www.aetna.comComplaint and Appeal Request NOTE: Completion of this form is mandatory. To obtain a review submit this form as well as information that will support your appeal, which may include medical records, office notes, discharge summaries, lab records and/or member history (this is not an all-inclusive list) to the address listed on your

UMR Post-Service Appeal Request Form
www.umr.comUMR Post-Service Appeal Request Form . Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by UMR. If you are appealing on behalf of someone else, please also include the Designation of Authorized Representative form with this request. 1. Today’s date:

Physician and Professional Provider Request For Claim ...
www.bcbstx.comRequest For Claim Appeal/Reconsideration Review Form Do not attach claim forms unless changes have been made from the original claim that was submitted. Please attach supporting documentation to facilitate your review, for example the operative report, or medical records, etc. This form must be placed on top of the correspondence you are ...

APPEAL REQUEST
esdorchardstorage.blob.core.windows.netAPPEAL REQUEST *Why do you disagree with the determination in the letter indicated above? ... We can’t accept your appeal without your signature. Print this page and submit once by fax or mail to the address listed below with any additional information you wish to provide. Visit your local WorkSource office if you need help faxing the appeal.
Request for Health Care Professional Payment Review
www.cigna.comIf a Customer Service representative is unable to change the initial decision, you will be advised at that time of your right to request an appeal. Step2: Complete and mail this form and/or appeal letter along with all supporting documentation to the address identified in Step 3 on this form.