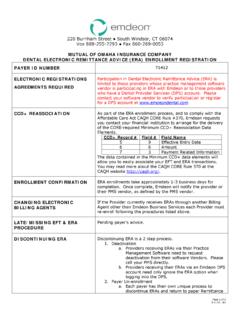
Transcription of EFT Contact Request Form - Emdeon
1 EFT Contact Request /UPDATE To add a new Contact to your existing epayment enrollment please provide: Complete the Provider Information section Provide Identifiers Information If you choose to assign a delegate, enter Contact information under the Delegated (New) Contact section Electronic copy of a government issued ID from all delegates (with signature), on payee legal entities letter head. This is to include the original authorized signature holder. To replace the existing EFT Contact : Complete the Provider Information section Provider Identifiers Information If you choose not to assign a delegate, leave the Delegated Contact section blank Electronic copy of a government issued ID (with signature), on payee legal entities letter head Authorized Signature section EFT Contact Request Provider NameDoing Buisness As Name (DBA)Provider AddressStreetCityState/ProvinceZip Code/Postal CodeProvider InformationProvider Federal Tax Identification Number (TIN) or Employer Identification Number (EIN)
2 Provider Identifiers Information Provider Contact NameTitleTelephone Number/ ExtEmail AddressFax NumberPro vider Contact NameTitleTelephone Number/ExtEmail AddressFax NumberProvi der Contact NameTitleTelephone Number/ExtEmail Address Existing Contact No longer at the Facility Delagated (New) ContactsAuthorized SignaturePrinted Title of Person Submitting EnrollmentSubmission Date Authorization SignaturePage 1 of 1 Questions? Call (Option 1) for SignatureAuthorized SignatureAuthorized Signature Fax NumberTelephone Number/ExtEmail AddressFax this form to 615-238-9615 or email it to