Transcription of Generic fax request form - Cigna
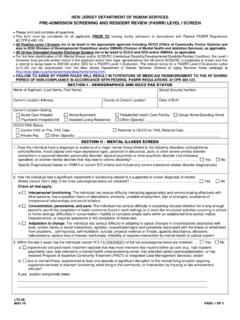
1 Generic fax request formProviders: you must get Prior Authorization (PA) for services before service is provided. PA is not guarantee of payment. Payment is subject to coverage, patient eligibility and contractual limitations. Please use appropriate form for Durable Medical Equipment (DME) and Home Health Care Please check request typeNote: If the service has already been provided, please follow retro process and submit certify that waiting for a decision under the standard time frame could place the enrollee s life, health, or ability to regain maximum function in serious jeopardy. Provider signature requiredPatient nameRequesting providerPatient ID #Provider NPI #Patient birthdate Contact nameContact phone #Contact fax #Date of serviceMA ONLY: Is provider part of a regulated facility?
2 Diagnosis with ICD 10 Service or procedure, including codesQuantity or number of visits requestedPCOMM-2023-316 Please fax this form and supporting clinical information to the appropriate contact listed below: For a list of services requiring PA, visit or call your state s Pre-Cert Department If you need help finding a PAR facility or provider, please call 800-230-6138 or visit and use the Provider Search requestExpedited request -May take up to 72 InpatientOutpatientAll Cigna products and services are provided exclusively by or through operating subsidiaries of Cigna Corporation. The Cigna name, logos, and other Cigna marks are owned by Cigna Intellectual Property, Inc. 963910 03/23 2023 CignaPhone # # HealthCareAllies Inpatient (TX)Part BPreferred Homecare (AZ DME)eviCorePost-Acute Care: Home Health: Oncology: Health Care Network (PHCN) (AZ Home Care) : MSK: High Tech Radiology: Therapy: Care: Home Health: Oncology: Therapy: : MSK: High Tech Radiology: of facility/place of service/specialist//