Transcription of Guideline: Venous thromboembolism (VTE) in pregnancy …
1 Refer to online version, destroy printed copies after use Page 1 of 24 Maternity and NeonatalClinical GuidelineQueensland Health Clinical Excellence Queensland Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium Refer to online version, destroy printed copies after use Page 2 of 24 Document title: Publication date: Document number: Document supplement: Amendments: Amendment date: Replaces document: Author: Audience: Review date: Endorsed by: Contact: VTE prophylaxis in pregnancy and the puerperium March 2020 The document supplement is integral to and should be read in conjunction with this guideline. Full version history is supplied in the document supplement.
2 Full review Queensland Clinical Guidelines Health professionals in Queensland public and private maternity and neonatal services March 2025 Queensland Clinical Guidelines Steering Committee Statewide Maternity and Neonatal Clinical Network (Queensland) Email: URL: Disclaimer This guideline is intended as a guide and provided for information purposes only. The information has been prepared using a multidisciplinary approach with reference to the best information and evidence available at the time of preparation. No assurance is given that the information is entirely complete, current, or accurate in every respect. The guideline is not a substitute for clinical judgement, knowledge and expertise, or medical advice.
3 Variation from the guideline, taking into account individual circumstances, may be appropriate. This guideline does not address all elements of standard practice and accepts that individual clinicians are responsible for: Providing care within the context of locally available resources, expertise, and scope of practice Supporting consumer rights and informed decision making, including the right to decline interventionor ongoing management Advising consumers of their choices in an environment that is culturally appropriate and whichenables comfortable and confidential discussion. This includes the use of interpreter services wherenecessary Ensuring informed consent is obtained prior to delivering care Meeting all legislative requirements and professional standards Applying standard precautions, and additional precautions as necessary, when delivering care Documenting all care in accordance with mandatory and local requirementsQueensland Health disclaims, to the maximum extent permitted by law, all responsibility and all liability (including without limitation, liability in negligence)
4 For all expenses, losses, damages and costs incurred for any reason associated with the use of this guideline, including the materials within or referred to throughout this document being in any way inaccurate, out of context, incomplete or unavailable. Recommended citation: Queensland Clinical Guidelines. Venous thromboembolism (VTE) in pregnancy and the puerperium. Guideline Queensland Health. 2020. Available from: State of Queensland (Queensland Health) 2020 This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives International licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute Queensland Clinical Guidelines, Queensland Health and abide by the licence terms.
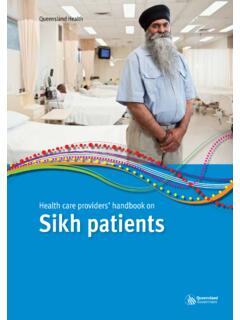
5 You may not alter or adapt the work in any way. To view a copy of this licence, visit For further information, contact Queensland Clinical Guidelines, RBWH Post Office, Herston Qld 4029, email For permissions beyond the scope of this licence, contact: Intellectual Property Officer, Queensland Health, GPO Box 48, Brisbane Qld 4001, email phone (07) 3234 1479. Cultural acknowledgement We acknowledge the Traditional Custodians of the land on which we work and pay our respect to the Aboriginal and Torres Strait Islander elders past, present and emerging. Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium Refer to online version, destroy printed copies after use Page 3 of 24 Flow Chart: VTE assessment for pregnant and postpartum women Flowchart: Perform VTE risk assessmentDevelop VTE prevention planMonitor and reassess riskPrepare for discharge/ ongoing careAdvise women of.
6 Increased risk of VTE in pregnancy and puerperium Signs/symptoms of VTE Importance of mobilising and avoiding dehydration Options and risks/benefits of prophylaxis As indicated by assessment Liaise with expert Offer/recommend prophylaxiso GCSo IPC or SCDo LMWH Discuss o Side effects of prophylaxiso Implications for birtho Ongoing risk of VTES igns and symptoms VTE PE: dyspnoea, palpitations/tachycardia, chest pain,haemoptysis, tachypnoea, hypotension, collapseDVT: unilateral leg pain, swelling in extremity, increase in calf circumference (more than 2 cm), increased temperature, prominent superficial veins, pitting odemaEarly in pregnancy assess: Personal/family history of VTE Presence of thrombophilia Known risk factors Medical comorbidities Contraindications to prophylaxis Signs/symptoms of VTER epeat assessment if: Antenatal hospital admission pregnancy complications Prolonged immobility Other change in risk statusIf prophylaxis indicated Plan intrapartum care (consider planned birth if indicated) Consider anaesthetic referral from 32 weeks Precautions for neuraxial blockadePostnatal risk Assess intrapartum or within 6 hours of birth Review VTE prevention plan and adjust as requiredAdvise women of.
7 Increased risk of VTE postpartum Signs/symptoms of VTE and seeking help Importance of correct use, application and duration of prophylaxis Implications for future pregnancyPharmacological prophylaxis Provide prescription for entire postnatal courseRefer as required For ongoing management GP follow-upAssess women on an individual basis. Liaise with a team experienced in prophylactic assessment and management as required DVT: deep vein thrombosis, GCS: graduated compression stockings, GP: general practitioner, IPC: intermittent pneumatic compressions, LMWH: low molecular weight heparin, PE: pulmonary embolism, SCD: sequential compression device, VTE: Venous thromboembolism , Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium Refer to online version, destroy printed copies after use Page 4 of 24 Flowchart.
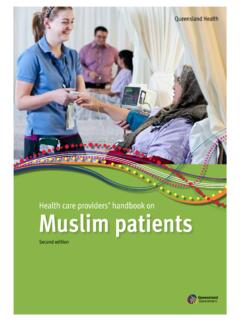
8 Antenatal and postnatal thromboprophylaxis according to risk High riskAll risk Family history (1st degree relative) of unprovoked or estrogen provoked VTE Single VTE provoked by surgery Age > 35 years Parity 3 Smoking (any amount) Gross varicose veins Current BMI 30 39 kg/m2 Current BMI 40 kg/m2 IVF/ART Multiple pregnancy Pre-eclampsia in current pregnancy Immobility Current systemic infection Pre-existing diabetes Caesarean section in labour Elective caesarean section Prolonged labour > 24 hours Operative vaginal birth Preterm birth (< 37+0 weeks) PPH > 1 L or transfusion Stillbirth in current pregnancy Caesarean hysterectomy1311111211111131111113 Antenatal risk scorePostnatal risk score = antenatal + postnatal score 4 LMWH standard prophylaxis From time of assessmentLMWH standard prophylaxis From 28 weeks3 Mobilise, avoid dehydrationALLAll caesarean sections Recommend IPC or SCD until next daySum all risk scores 5 SELECT ALL THAT APPLY at every assessment (antenatal or postnatal)Risk ScoreANY ONE OF Antenatal hospital admission Ovarian hyperstimulation syndrome (first trimester only) Any surgery ( pregnancy or postpartum)
9 Severe hyperemesis or dehydration requiring IV fluidLMWH Standard prophylaxis While in hospital or until resolves4IF THROMBOPHILIA High or low risk thrombophilia* (no personal history VTE)Refer to Flowchart: VTE prophylaxis if thrombophilia3 ANY ONE OF Any single previous VTE not provoked by surgery Recurrent provoked VTE (2 or more) Active autoimmune or inflammatory disorder Medical co-morbidity: ( cancer, nephrotic syndrome, heart failure, sickle cell, type I diabetes with nephropathy)LMWH standard prophylaxis From first trimester Continue 6 weeks postpartum2 ANY ONE OF Pre- pregnancy therapeutic anticoagulation (any reason) Any previous VTE plus high risk thrombophilia*# Recurrent unprovoked VTE (2 or more) VTE in current pregnancy (seek expert advice)Therapeutic anticoagulation Continue/commence antenatal Continue 6 weeks postpartum# High prophylactic dose may be appropriate1 Mobilise early, avoid dehydrationALLLMWH standard prophylaxis Until discharge 2 LMWH standard prophylaxis 7 days (or longer if ongoing risk) 3* High risk thrombophilia.
10 > 1 laboratory thrombophilia, APS, antithrombin deficiency, protein C deficiency, protein S deficiency, homozygous FVL, homozygous prothrombin mutation, compound heterozygous FVL/prothrombin mutation Low risk thrombophilia: heterozygous FVL, heterozygous prothrombin mutation, antiphospholipid antibodiesGCS/TED stockings Consider for postnatal women until fully mobile Recommend if receiving LMWHE noxaparin: standard prophylaxis (subcut) 50 90 kg 40 mg daily 91 130 kg 60 mg daily 131 170 kg80 mg daily > 171 kg mg/kgFlowchart: APS: antiphospholipid syndrome, ART: artificial reproductive technology, BMI: body mass index, FVL: factor V Leiden, GCS: graduated compression stockings, IPC: intermittent pneumatic compressions, IVF: in-vitro fertilisation, LMWH: low molecular weight heparin, PE: pulmonary embolism, PPH: Primary postpartum haemorrhage, SCD: sequential compression device, SLE: systemic lupus erythematosus, TEDS: thromboembolic deterrent stockings VTE: Venous thromboembolism , : greater than or equal to, >: greater than Queensland Clinical Guideline: VTE prophylaxis in pregnancy and the puerperium Refer to online version, destroy printed copies after use Page 5 of 24 Flowchart: Thromboprophylaxis if thrombophilia APS: antiphospholipid syndrome, BD: twice daily, >: greater than : greater than or equal to POSTNATALANTENATALAny of.