Example: biology
HMSA PRECERTIFICATION REQUEST Please fax completed …
Subscriber’s name (last, first, MI) Phone no. B. ICD-10-CM diagnosis code(s) Diagnosis code(s): C. Procedure/service/treatment information. Place of service: Inpatient Outpatient/ASC (ambulatory surgical center) Labs and diagnostic services (outpatient) Office Home
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

Electroconvulsive Therapy (ET)
hmsa.comElectroconvulsive Therapy (ET) BEACON HEALTH STRATEGIES, LLC ORIGINAL EFFECTIVE DATE HAWAII LEVEL OF CARE CRITERIA 2013 CURRENT EFFECTIVE DATE 2016 I. Description Electro-Convulsive (ECT) Therapy is a procedure in which an electric current is …

Cytochrome p450 Genotyping - 9/1/16
hmsa.comThe cytochrome p450 (CYP450) family is a major subset of all drug-metabolizing enzymes; several CYP450 enzymes are involved in the metabolism of a significant proportion of …

Hematopoietic Stem-Cell Transplantation for Multiple ...
hmsa.comHematopoietic Stem-Cell Transplantation for Multiple Myeloma 2 graft-versus-malignancy (GVM) effect mediated by non-self immunologic effector cells that develop after engraftment of allogeneic stem cells within the patient’s bone marrow space.

Hawaii Medical Service Association
hmsa.comCreated Date: 12/31/2021 6:14:43 AM

HMSA Quest Integration member handbook
hmsa.com2 HMSA QUEST Integration: (808) 948-6486 or 1 (800) 440-0640 • TTY: 1 (877) 447-5990 • hmsa.com/QUEST. Important Information About Your Health Plan
Related documents

REGISTERED EDUCATION SAVINGS PLAN (RESP) TRANSFER …
www.canada.caTo be completed by the subscriber PROTECTED WHEN COMPLETED - B. Page 1 of 4 Emploi et Développement social Canada. Employment and Social Development Canada. REGISTERED EDUCATION SAVINGS PLAN (RESP) TRANSFER FORM Part A: Subscriber request. This form is valid only if completed, signed, dated and given to the receiving RESP promoter.

Federal Reserve Bank Subscriber Access Request Form for …
www.frbservices.org**A separate form MUST be completed for each legal entity** Section 1 – General Information Please Check One New Subscriber – Subscriber is a new user to Reporting Central Delete Subscriber – Subscriber no longer needs access to Reporting Central* Add Access – Add access for Subscriber as listed in Section 3

AUTHORIZATION FOR DISCLOSURE OF PROTECTED HEALTH …
www.cigna.comSubscriber Name (if different from Customer): Subscriber’s Employer: Subscriber’s Relationship to Customer: Subscriber’s Social Security # (if different from customer) (Optional): If you have additional coverage with Cigna, other than that which is described above, please provide the ... HealthCare, another form will need to be completed ...

BURGLAR & FIRE ALARM SUBSCRIBER / PROPRIETOR …
www.phoenix.govSUBSCRIBER / PROPRIETOR INFORMATION Please Print Clearly or Type ( ) Name of Residence or Name of Business (Should be Same Name Alarm Company Uses for Dispatch) Telephone Number At Location ... wait for a emailn ed response, and then 602call -534-0322 (or fax the completed application, wait 60 minutes, and then call 602-534-0322). APPLICANT ...
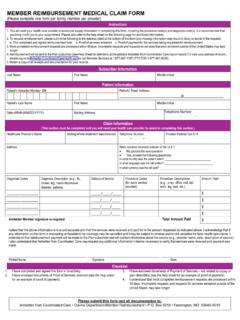
MEMBER REIMBURSEMENT MEDICAL CLAIM FORM
ambetter.coordinatedcarehealth.com3.Most completed reimbursement requests are processed within 45 days. Incomplete requests and requests for services that were rendered outside of the United States may take longer. 4.Reimbursement will be sent to the Plan subscriber (see Help Sheet for definition) at the address Ambetter from Coordinated Care has on record (To view your address ...

Over-the-Counter (OTC) At-home COVID-19 Test …
www.uhcsr.comcompleted form. If we don’t receive the required information, your request will not be processed. Information about the member who used the OTC COVID-19 Test Full name _____ What is your relationship to the subscriber/policyholder?