Example: stock market
Important Instructions for Completing This Form
*APP30504-05=02* Are you affiliated with or employed by a stock exchange or member firm of an exchange or FINRA, or a municipal securities broker-dealer?
Information
Domain:
Source:
Link to this page:
Documents from same domain

Important Instructions for Completing This Form
client.schwab.comImportant Instructions for Completing This Form For international clients: international.schwab.com | +1-415-667-8400 The form you requested follows this page. You can either complete it on your computer and then print it out, or print it out first and fill it in by hand. Please complete the form in English.

Schwab MoneyLink® Electronic Funds Transfer Form
client.schwab.comElectronic Funds Transfer Form Important Eligibility Information Organization or Corporate Accounts • If the account at the other financial institution is a corporation, partnership, sole …

Schwab Individual 401(k) Plan
client.schwab.comComplete the Summary Plan Description (SPD) in accordance with the elections you made on the Adoption Agreement. 2. Provide a photocopy of the completed SPD to each participant.

When your funds are available - Charles Schwab Corporation
client.schwab.commay not be immediately available for withdrawal. Schwab Bank is not responsible for delays in funds availability caused by other financial institutions.

Open a Schwab IRA
client.schwab.com* If you provide a Trusted Contact Person(s) to Schwab, you understand that you have authorized Schwab and your advisor (if you have one) to contact the Trusted Contact Person(s) at their discretion and to disclose information about

Important instructions for completing this form
client.schwab.comwww.schwab.com 1-800-435-4000 Important instructions for completing this form The form you requested follows this page. You can either complete it on your computer and

Request a Required Minimum Distribution - Schwab
client.schwab.comRequest a Required Minimum Distribution From Your Schwab IRA. Page 1 of 8. www.schwab.com 1-800-435-4000 (inside the U.S.) +1-415-667-8400 (outside the U.S.) 1-888-686-6916 (multilingual services) When to use this form: • Complete this form if you wish to take a Required Minimum Distribution (RMD) from your account.

Add Options Trading and Margin to Your Account
client.schwab.comaccountolder, h agent or attorney-in-fact, trustee, and/or authorized agent on the account will be able to engage in optionsrading. t ... Weespect r your privacy. ... andead r a copy of the Margin Disclosure Statement.

Move Assets from My Schwab Brokerage Account
client.schwab.comReturn the completed form by using Secure Messaging on www.Schwab.com or www.SchwabAlliance.com or Fax to 888-526-7252. Please use this form to move (or transfer) cash and/or assets from your Schwab brokerage account to another Schwab brokerage account(s). Please use a separate form for each originating account.

Designated Beneficiary Plan Agreement
client.schwab.comDesignated Beneficiary Plan Agreement Page 3 of 11 3. Instructions and Important Information In the event of my death, pay the full value of my account (in equal proportions, in the case of multiple beneficiaries, unless I indicate otherwise) to the Primary Beneficiary(ies) as designated in the Beneficiary Designation section below.
Related documents

SAMPLE CLIENT ENGAGEMENT LETTER
www.gabar.orgSAMPLE CLIENT ENGAGEMENT LETTER RE: .. [ Subject ] Dear [ Name ]: The purpose of this letter is to confirm, based on our conversation of [ date ], that [ insert firm name ] will represent
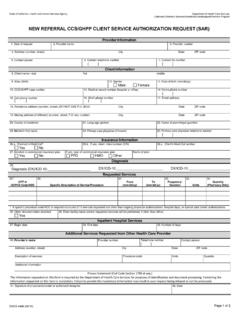
New Referral CCS/GHPP Client Service Authorization Request ...
www.dhcs.ca.govDHCS 4488 (09/15) Page 2 of 2 . Instructions. 1. Date of the request: Date the request is being made. Provider Information. 2. Provider’s name: Enter the name of the provider who is requesting services.

Practitioner/Clinic Name: Health Information
www.abmp.comAssociated Bodywork & Massage Professionals MEMBER Practitioner/Clinic Name: _____ Health Information Contact Information: _____ (page 1 of 2) Client Contact Information

ESTABLISHED CCS/GHPP CLIENT SERVICE AUTHORIZATION …
www.dhcs.ca.govINSTRUCTIONS 1. Date of the request: Date the request is being made. Provider Information 2. Provider’s name: Enter the name of the provider who is requesting services.

Client Name: Date Details
www.abaresources.comABA Progress Notes Client Name: Date Details www.abaresources.com