Transcription of Information about t he sanofi-aventis U.S. Patient ...
1 1. F2. TL3. Ai4. Han5. Fp sasaPPF Once you If prescriable to re Call 800-Fill out all ofTake the appLicensed PraAttach a copncome such Have the phaventis number abovFinally, mailphotocopy of Patient m Patient cAdministcoverageplease ap Patient ca Patient s Box 759 Phone (800) 2 Fax (866) 734 Informatiu qualify, yoibed, up to aefill your ord-221-4025 anf the informaplication to yactitioner (Npy of your F as paystubshysician fill brand namve. l or fax the f Federal incmust be a rescannot have tration, or ae. If the patpply as sanofannot have atotal yearly Househ123456s Patient Asss PatienSomerville, 221-4025 4-7372 on about thou may be aba 90 day suppder every 3 mnd use the auInstrucation in the ayour physiciNo stamped sFederal Tax s, a bank statout the Preme product. applicationcome tax retuPatieident of the or qualify fany state ortient has Mfi-aventis private phousehold i hold Size 1 2 3 4 5 6+ sistance Founnt Assistance NJ 08876 he sanofi -able to receiveply of medicmonths untilutomated syctions for capplication aan.)
2 Have yoignatures) . Return. If tement of description Se You can s, prescriptiourn (or otherent AssistaUnited Statefor any govr local progedicare may be abprescription income mustTotal Househo$ $ $ $ $ $ ndation Program aventis free mediccation will b the 12 montystem to refilcompletingand sign on tour physicia you do not posit, or an ection belowsee a complon (if not usr proof of inance Prograes. vernment pregrams. Patt D but is stble to coverat be at or belYearly old Income 27,225 36,775 46,325 55,875 65,425 74,975. Patient Acation for up e sent to youths is complll your medi the applicthe line that an sign on thfile taxes pattested lettew or includelete list of asing Prescripncome) to theam Eligibilescription cotient cannottill having age.
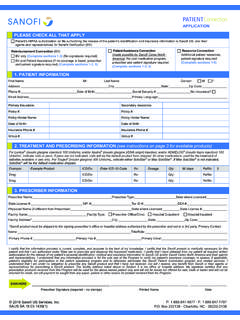
3 Low the limitTotal Househo233456 Assistance Pto 12 monthur healthcarelete. cation. cation says Patienhe line that splease includer describinge an originalavailable proption Sectione address or lity overage such have Meda problem ats shown in tMonthly old Income ,269 ,065 ,860 ,656 ,452 ,248 Program hs. e practitionent s signaturays Originade another pg your yearlyl prescriptiooducts by cn on the appfax number h as, Medicicare Part Daffording thethe chart belr. You will e . al Signature proof of yeary income. on of a sanoalling the 8plication), aabove. caid, VeteranD prescriptieir medicatiolow: be of rly ofi-800 and n s ion on, PATIENAMADDCITYDATDO YPRO AREIf noSOCWHA(IncluHOWP atient CPatient Nand accurDoctor/Hedoes not gand (3) peaventis Fodetermini(public/prrequired fand HIV tadministeregulationnot be abapplicatioterminate recordkeeagents froas long asaventis Fo PATIENTLICENNAMOFFICITYSTATOFFIPRESP roduProduTo the bepublic ( pright to mprescriptioreturned f LICENsaPPENT SECTME: (FirstDRESS: Y: TE OF BIRTHYOU HAVE GRAM?)))
4 VeteE YOU A , please descIAL SECURIAT IS YOUR uding Social W MANY PECertification and AName:_____rate and that I meeealthcare Providerguarantee that assieriodic re-applicatioundation for Pating my participatiorivate) or others. for participation intest results or diager the Program, orns. I agree that thible to participate inon as required. I mmy participation eping purposes. I om any and all clais such use or discoundation for PatieT S SIGNATURENSED PRAME: ICE ADDREY: TE LICENSEICE PHONE SCRIPTIONuct Name: uct Name: est of my knowledg. Medicaid), andparticipation of thmodify or terminaon products receivfor credit. I agree tNSED DR OR OTanofi-aventis Box 759 SPhone (800) 22 ION The t) H: OR QUALIF Mran s Admini. RESIDENT cribe your resiITY NUMBER TOTAL ANSecurity, PenOPLE ARE TAuthorization to _____et all eligibility crir if my income oristance will be obtion is required forient Assistance anon in, and adminisI authorize and cn the Program.
5 Mgnosis, if as required by lais authorization is n this Program. Umay withdraw this in this Program ahereby release, foims or liability arisclosure is made in ent Assistance reseE ACTITIONE SS: (No E NUMBER: #: N INFORMAdge the informationd meets the requireis Patient , I will alate this program aved from this Progto participate in anTHER HCP (No Patient AssistSomerville, NJ21-4025 Fax ( Patient or h FY FOR A PUMedicaid: Yistration: YT? YES Nidency statusER:_____NNUAL HOUnsion income,THERE IN YDisclose Informa_____iteria for participatr insurance status tained, and (1) parr continued participnd authorized thirdstering, the Prograconsent to release My authorization in. I understand thataw. I understand voluntary and thatUnless revoked thauthorization at aand will not affector myself and on bsing from their congood faith and werve the right at an Date ER SECTIO Box) ATION n contained in thised income limits flert Program Sponat any time withougram will be usedny recall of the prostamps) ance FoundatJ 08876 (866) 734-7372his/her legal(Middle) STATE: PHONE NUUBLIC OR PRYES NO YES NO NO Ar: _-_____-__USEHOLD IN, etc.)
6 : YOUR HOUSE ation _____ states thattion in the programchanges during thrticipation in this Ppation. I understand party agents invam, which may inof identifiable inncludes release of t identifiable informthat Information It I may refuse to shis authorization sany time by writtet Information alreabehalf of my succnduct pursuant to twithout malice andny time and withouON The lic StrengStrengs application is comfor participation innsor. I understand ut notice. I attesd for the above naoduct initiated by thtion 2 l representa UMBER: RIVATE PRE Medica re you current _____NCOME? EHOLD? t the Information m, including incomhe course of my paProgram is subjectnd that my informvolved in administclude contacting mnformation about minformation relatinmation about me wI authorize to be dign this authorizathall remain in effen notification to mady disclosed.
7 I essors and assignsthis authorization d is consistent withut notice to modifycensed pracPROFESSIOSTATE: OFFICE CONOFFICE FAXgth: gth: mplete and accuran this Program. If that sanofi -aventist that I am not omed Patient only he manufacturer. ative must c(Las ZIP COD ESCRIPTIONare Part D: Y Othertly a member __ $ 1 2 and documents prme limits. I agreearticipation in thist to approval undemation will be used tration of this Progme as well as my me including medng to treatment fowill be kept confiddisclosed may be tion. Refusal to sifect throughout mmy Doctor/Healthfurther authorize us, Program Sponsoor the use or discloh this authorizatioy or change eligibictitioner muONAL DESIG ZIPNTACT PERX #: QQate and this patientI become aware ois and the sann the HHS/OIG land will not be re Dcomplete thist) E: N DRUG BENYES NO r State or Locof Together 3 4 rovided in connece to immediately ins Program.
8 I under Program guideliby the Program Sgram, (collectivelyDoctor/Healthcaredical, financial andr substance abusedential and will nore-disclosed and nign will not affect my participation in hcare Provider; house of my Social or (collectively), tosure of Information . I understand tility criteria, or moust completeGNATION: (MP CODE: RSON: Quantity Per DQuantity Per Dt has no prescriptiof a change in inconofi-aventis Foundlist of Excluded Iesold nor offered fDate is section Gender:NEFIT OR IN Private:cal Programs:Rx? YES 5 6+ction with this appnform a Program rerstand that applicnes, (2) approval iponsor, sanofi -avey Program Sponse Provider, office/d insurance record, psychiatric and/oot be further used no longer protectemy ability to obtathe Program, inclwever withdrawalSecurity number their officers, direcon relating to my that sanofi -aventisodify or discontinue this sectionMD, DO, ETC Day: Day: ion insurance coveome or insurance dation for Patient AIndividuals.))
9 My sifor sale, trade or b M F NSURANCE : YES NO YES NONO + plication are comprepresentative andcation to the Progis for a limited perentis, , the sansor ), for purpose/hospital staff, insds and informationor medical conditior disclosed exceped by Federal privain treatment but I luding subsequentl of authorization for identification ctors, employees, Program participas and the sanue this Program. n C.): erage either privatstatus that may efAssistance reserveignature certifies barter and will no plete d my gram riod nofi-es of urer n as ons, pt to vacy will t re-will and and ation nofi-te or ffect e the that ot be