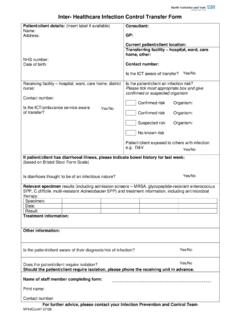
Transcription of Inter-facility Infection Control Transfer Form
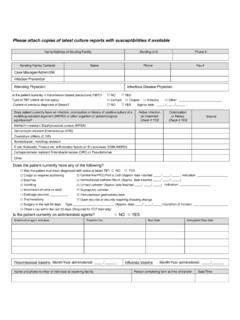
1 Inter-facility Infection Control Transfer Form 7 KLV IRUP PXVW EH ILOOHG RXW IRU WUDQVIHU WR DFFHSWLQJ IDFLOLW\ ZLWK LQIRUPDWLRQ FRPPXQLFDWHG SULRU WR RU ZLWK WUDQVIHU Please attach copies of latest culture reports with susceptibilities if availableSending Healthcare facility : 3 DWLHQW 5 HVLGHQW /DVW 1 DPH )LUVW 1 DPH 'DWH RI %LUWK 0 HGLFDO 5 HFRUG 1 XPEHU BBB BBBB BBBBBBB 1 DPH $GGUHVV RI 6 HQGLQJ )DFLOLW\ 6 HQGLQJ 8 QLW 6 HQGLQJ )DFLOLW\ SKRQH 6 HQGLQJ )DFLOLW\ &RQWDFWV 1$0( 3+21( ( PDLO &DVH 0 DQDJHU $GPLQ 6: ,QIHFWLRQ 3 UHYHQWLRQ Is the patient currently in isolation?
2 NO YES Type of Isolation (check all that apply) Contact Droplet Airborne Other: _____ Does patient currently have an Infection , colonization OR a history of positive culture of a multidrug-resistant organism (MDRO) or other organism of epidemiological significance? Colonization or history Check if YES Active Infection on Treatment Check if YES Methicillin-resistant Staphylococcus aureus (MRSA) Vancomycin-resistant Enterococcus (VRE) Clostridium difficile Acinetobacter, multidrug-resistant* E coli, Klebsiella, Proteus etc.
3 W/Extended Spectrum %-Lactamase (ESBL)* Carbapenemase resistant Enterobacteriaceae (CRE)* Other: Does the patient/resident currently have any of the following? &RXJK RU UHTXLUHV VXFWLRQLQJ &HQWUDO OLQH 3,&& $SSUR[ GDWH LQVHUWHG BBB BBB BBBBB 'LDUUKHD +HPRGLDO\VLV FDWKHWHU 9 RPLWLQJ 8 ULQDU\ FDWKHWHU $SSUR[ GDWH LQVHUWHG BBB BBB BBBBB ,QFRQWLQHQW RI XULQH RU VWRRO 6 XSUDSXELF FDWKHWHU 2 SHQ ZRXQGV RU ZRXQGV UHTXLULQJ GUHVVLQJ FKDQJH 3 HUFXWDQHRXV JDVWURVWRP\ WXEH 'UDLQDJH VRXUFH BBBBBBBBBBBBBBBBBBBBBBBBBBBB 7 UDFKHRVWRP\ Is the patient/resident currently on antibiotics?]]
4 NO YES: Antibiotic and dose Treatment for: Start date Anticipated stop date Vaccine Date administered (If known) Lot and Brand (If known) Year administered (If exact date not known) Does Patient self report receiving vaccine? ,QIOXHQ]D VHDVRQDO oyesono3 QHXPRFRFFDO oyesono2 WKHU BBBBBBBBBBBBB oyesonoPrinted Name of Person completing form Signature Date If information communicated prior to Transfer : Name and phone of individual at receiving facility