Transcription of Keeping Dementia Residents Safe - Assisted Living Consult ...
1 Keeping Dementia Residents safe Anne Ellett, NP, MSN. A ssisted Living (AL) opera- tors face many challenges when it comes to provid- ing good care to Residents with cognitive impairment. Unsafe events in their own homes, such as falls, injuries, medication mis- management, and episodes of wandering, are often the precipi- tating factors that motivate a family to recommend that their loved one move to an AL environment. In one recent survey, it was re- ported that of AL properties are licensed for Dementia care. Even in those AL properties not li- censed for Dementia care, there are many Residents with some de- gree of cognitive impairment re- quiring extra monitoring and assis- tance with activities of daily Living (ADLs). The typical AL resident needs assistance with ADLs (bathing, dressing, transferring, toi- leting, and eating). The average One-on-one caregiver Lucy Czaykowska and resident Ernie Fybel share a quiet moment at Silverado, Encinitas.
2 Photo courtesy of Silverado Senior Living . age of AL Residents is years old1 and with age comes increasing risk of cognitive impairment. Near- Wandering and Elopement by a cognitively impaired and dis- ly 1 out of 2 people older than 85 Wandering and elopement is every oriented individual characterized has Alzheimer's or other form of AL operator's nightmare situation. by excessive ambulation, leading This behavior is common in people to safety and/or nuisance-related Residents with cognitive impair- with Dementia , and the Alzheimer's Even though Residents ment have special safety concerns. Association reports that more than may have Dementia , their behav- They are especially vulnerable be- 60% of people with Alzheimer's dis- ior can be very purposeful. De- cause they may not be able to artic- ease wander at some point. There- mentia Residents often have a goal ulate their needs. In particular, fore, there is a high probability that in mind (to return home, find there are 4 specific areas of safety many Residents Living in your AL their children, go to their former concern for those Dementia resi- community are at risk for wandering work site) and search over and dents Living in an AL setting: and elopement.
3 And many Residents over again for a way to get to Risk for wandering and elopement wander repeatedly. their destination. Falls and injuries Wandering is not just aimless An example is a resident who Challenging behaviors movement. Wandering is defined was Living in a Dementia -specialty Polypharmacy as purposeful behavior initiated AL facility and eloped 2 times. September/October 2007 Assisted Living Consult 19. Each time he had the same goal there have been previous episodes year, and of those who fall, 20% to to get to city hall to obtain a mar- because they fear the facility won't 30% suffer moderate to severe in- riage license for him and his fa- allow their loved one to move in. There aren't any published vorite female staff person to get Map the resident 's behavior for reports of the frequency of falls in married. By closely following a vis- an initial period (3 to 14 days are AL, but one study of continuing itor out of the security-coded front recommended) to provide detailed care retirement communities indicat- door, he was able to get several information about the new resi- ed a fall rate of 56% ,6.
4 Miles away. He kept asking for di- dent's activities and any triggers for The average age of Residents in rections from passersby and even- elopement-seeking behavior. AL facilities is years old,1 so it tually did arrive at the local city Training of associates is constant is no surprise that falls and injuries hall. An astute clerk there noticed and ongoing. Train staff how to re- are a frequent occurrence. Demen- his general level of confusion and spond to door alarms, and make tia Residents are at increased risk of some printed literature in his coat sure they know which Residents are falls because of their judgment im- pocket. Luckily it was a brochure at risk for elopement. Educate staff pairment and often other accompa- of his AL community. Phone calls about how to redirect Residents nying risk factors such as altered were made, and he was safely re- away from the exits and engage gait and sensory deficits. turned. This AL community learned them in desirable activities.
5 Make The greatest predictor of a fall is that even a very confused person sure staff regularly check on high- a previous fall. If the AL staff ob- can, if he or she focuses on a goal, risk Residents to determine their tains information from the family often successfully figure out a way whereabouts. Ensure that photo IDs that there is a history of previous to elope, even from a secured en- falls, they can identify that resident vironment. as high risk. Some other risk factors If a resident is successful in to consider are: elopement and is injured, expen- Lower extremity weakness sive liability claims may follow. Gait disorders and decreased Common allegations in these suits Even a very confused range of motion (ROM). include failure: person can, if he or she Inability to transfer to a chair To hire sufficient staff to ade- focuses on a goal, often without assistance quately supervise Residents Associated medical conditions, To train professional staff to successfully figure out such as cardiac impairment or properly supervise Residents a way to elope.
6 Parkinson's disease To employ alarms or other de- Polypharmacy vices to prevent elopement Use of psychotropic medications Of staff members to properly re- Visual impairment spond to alarms Incontinence of all Residents are available, assign Development of a policy and pro- designated search areas to individ- The challenge for AL facilities is cedure for assessment of elopement ual staff members, determine a Keeping Dementia Residents safe risk and an emergency missing resi- timeframe in which the administra- from injuries but allowing them the dent plan can help minimize the tor and family are to be contacted dignity of choice in an environment risk for elopement and injury. and when the local police are to be that is as unrestrictive as possible. The greatest risk period for resi- notified, and conduct drills on a These goals may seem contradicto- dent elopement is often in the ini- regular basis with all shifts. ry. Is maximizing independence tial transition to the AL.
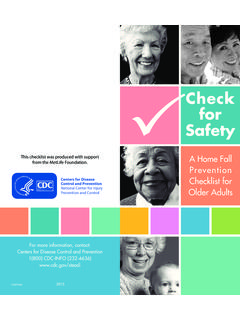
7 In the new Also ensure that all exits are and choice inconsistent with pre- environment the resident may be clearly in view and alarms and venting falls and fractures? anxious, mistrust staff, and explore cameras are in place. Post staff in At Silverado Senior Living , we all areas of the AL for an opportu- view of all exit areas. have been very successful in Keeping nity to elope. fall and fracture rates low through a Fall and Injury Prevention focused fall and injury prevention resident Assessment for Risk of falls and injuries is another program (Figures 1 and 2). Elopement Risk area of safety concern for all elderly Because the cause of most falls Directly ask the family if there have adults, but especially so for resi- is multifactorial, Silverado Senior been any episodes of wandering and dents with Dementia . Falls are the Living includes several key compo- elopement prior to admission to help most frequent cause of injury in nents in their fall and injury pre- identify high-risk Residents .
8 Often older adults. Thirty-three percent of vention program: families are hesitant to mention that adults ages 65 and older fall each Universal precautions: ALL resi- 20 Assisted Living Consult September/October 2007. (ADRs) that are directly related to the numbers of medications taken. Figure 1. The risk of ADRs rises exponen- Injury rate from falls at Silverado Senior Living tially as the number of drugs in- creases (Figure 5). 30%. A person's ability to absorb and 27%. 25%. metabolize numerous medication 22%. decreases with age. A recent study 20% showed that the average number of 17% medications taken by an AL resi- 15% dent is Residents with demen- 12% tia often take many more than the 10% more independent Residents and are unable to tell staff if they are 5%. feeling poorly from the medica- 0%. tions. Excessive medications that 1909 2000 2001 2002 2003 2004 2005 2006 can contribute to the risk of falls, such as psychotropic medications, sleeping medications, and seda- tives, are sometimes given to help staff deal with difficult behaviors Figure 2.
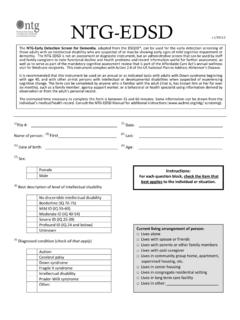
9 Such as yelling, wandering, aggres- Fracture rate at Silverado Senior Living sion, or other antisocial behaviors in Dementia Residents . Antihyper- 7% tensive agents and other cardiac 6%. 6% medications may also cause changes in pulse and blood pres- 5%. sure and symptoms such as light- 4% headedness or dizziness. Because 3% Dementia Residents are especially 3%. vulnerable to polypharmacy, it is 2%. 2% helpful to have nursing or other 1% 1% 1% trained staff review all medications 1% on a regular basis and work with 0% the family and physicians to appro- 1909 2000 2001 2002 2003 2004 2005 2006. priately reduce and discontinue medications no longer beneficial. Altercations between Residents or dents are viewed as high-risk prevent deconditioning (Figures between staff and Residents can fall candidates because of their 3 and 4) lead to injuries. Managing these be- Dementia Use of hipsaver garments by haviors can be very difficult for the Extensive and on-going training most high-risk Residents staff.
10 However, before any such of all staff (including culinary, Regular review of medications to medications are added, it is helpful housekeeping, activities, and avoid sedation or other drug-re- for the staff to behavior map the leadership staff) regarding risk lated adverse effects that can resident to determine what might factors for falls and which resi- contribute to falls be triggering these challenging be- dents were at highest risk Review of every fall to determine haviors. Behavior mapping notes Scrutiny of the environment for contributory factors where the resident is and what the any factors that may contribute resident is doing every 15 to 30. to resident falls Polypharmacy minutes for 24 to 72 hours. Often a Increased use of physical thera- By definition, polypharmacy pattern of behavior can be discov- py and restorative care to im- means many drugs. Elderly adults ered. For example, aggressive be- prove gait and increase transfer use more drugs because illness is havior may show up more often skills more common in older persons.