Transcription of MCMI-III Interpretive Report
1 MCMI -III Millon Clinical Multiaxial Inventory-III Interpretive Report with Grossman Facet Scales Theodore Millon, PhD, DScName: Joan Sample ID Number: 12566 Age: 44 Gender: Female Setting: Outpatient Never Hospitalized Race: White Marital Status: Divorced Date Assessed: 11/30/2014 Copyright 1994, 2005, 2009 DICANDRIEN, Inc. All rights , the PSI logo, and PsychCorp are trademarks in the and/or other countries of Pearson Education, Inc., or its affiliate(s). MCMIand Millon are registered trademarks of DICANDRIEN, Inc.
2 DSM-IV is a registered trademark of the American Psychiatric SECRET INFORMATIONNot for release under HIPAA or other data disclosure laws that exempt trade secrets from disclosure.[ / RE1 / QG1 ]SAMPLE9588 CAPSULE SUMMARYMCMI-III reports are normed on patients who were in the early phases of assessment or psychotherapyfor emotional discomfort or social difficulties. Respondents who do not fit this normative population orwho have inappropriately taken the MCMI-III for nonclinical purposes may have inaccurate reports. TheMCMI-III Report cannot be considered definitive.
3 It should be evaluated in conjunction with additionalclinical data. The Report should be evaluated by a mental health clinician trained in the use ofpsychological tests. The Report should not be shown to patients or their ConsiderationsThe client is a 44-year-old divorced white female. She is currently being seen as an outpatient, and shedid not identify specific problems and difficulties of an Axis I nature in the demographic portion of patient's response style may indicate a tendency to magnify illness, an inclination to complain, orfeelings of extreme vulnerability associated with a current episode of acute turmoil.
4 The patient's scalescores may be somewhat exaggerated, and the interpretations should be read with this in SeverityOn the basis of the test data, it may be assumed that the patient is experiencing a severe mentaldisorder; further professional observation and inpatient care may be appropriate. The text of thefollowing Interpretive Report may need to be modulated upward given this probable level of DiagnosesShe appears to fit the following Axis II classifications best: Negativistic (Passive- aggressive )Personality Disorder, and Borderline Personality Disorder, with Dependent Personality Traits, andAvoidant Personality I clinical syndromes are suggested by the client's MCMI-III profile in the areas of MajorDepression (recurrent, severe, without psychotic features), Generalized Anxiety Disorder, andPosttraumatic Stress ConsiderationsInconsistent and pessimistic, this patient may expect to be mishandled, if not harmed, even bywell-intentioned therapists.
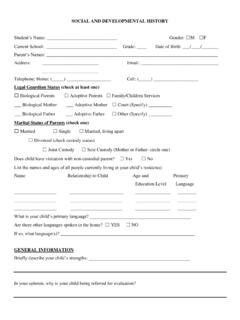
5 Sensitive to messages of disapproval and lack of interest, she may complainexcessively and be irritable and erratic in her relations with therapists. Straightforward and consistentcommunication may moderate her dependent/negativistic attitude. Focused, brief treatment approachesare likely to overcome her initial oppositional -III Interpretive Report ID: 1256611/30/2014, Page 2 Joan SampleSAMPLEDISCLOSUREDESIRABILITYDEBASE MENTSCHIZOIDAVOIDANTDEPENDENTHISTRIONICN ARCISSISTICANTISOCIALSADISTICCOMPULSIVEN EGATIVISTICMASOCHISTICSCHIZOTYPALBORDERL INEPARANOIDANXIETYSOMATOFORMBIPOLAR.
6 MANICDYSTHYMIACATEGORYSCOREPROFILE OF BR SCORESDIAGNOSTIC SCALESMODIFYINGINDICESRAWBRSEVEREPERSONA LITYPATHOLOGYCLINICALPERSONALITYPATTERNS CLINICALSYNDROMESALCOHOL DEPENDENCEDRUG DEPENDENCETHOUGHT DISORDERMAJOR DEPRESSIONDELUSIONAL DISORDERINVALIDITY (SCALE V) =INCONSISTENCY (SCALE W) =DEMOGRAPHIC CODE:PERSONALITY CODE:SYNDROME CODE:XYZ13456B78A8 BSCPAHNDBTSSCCPP932057169465163908393124 0666593689766718868767010063413227121414 8241316231517131117814172178A 3 ** 2A 2B * 6A 8B 1 + 6B 5 " 7 4 ' ' // C ** - * //A D ** T R * // CC ** - * //0412566/ON/F/44/W/D/-/--/--/------/--/ ------/6220607585115 MILLON CLINICAL MULTIAXIAL INVENTORY - IIICONFIDENTIAL INFORMATION FOR PROFESSIONAL USE ONLYDEPRESSIVE2A2B6 ARPOST-TRAUMATIC STRESS02076188328 SEVERECLINICALSYNDROMESMCMI -III Interpretive Report ID.
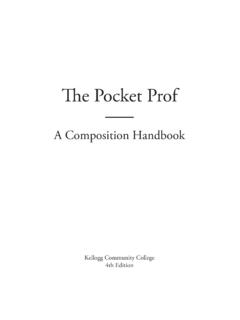
7 1256611/30/2014, Page 3 Joan SampleSAMPLESCALESCORE93 PROFILE OF BR SCORES9885 RAWBR865 HIGHEST PERSONALITY SCALE BR 65 OR HIGHER: SCALEMILLON CLINICAL MULTIAXIAL INVENTORY - IIIFACET SCORES FOR HIGHEST PERSONALITY SCALES BR 65 OR Self-ImageExpressively ResentfulTemperamentally PERSONALITY SCALE BR 65 OR HIGHER: SCALEPROFILE OF BR SCORESFACET SCALESCT emperamentally LabileInterpersonally ParadoxicalUncertain SCALESPROFILE OF BR SCORESBRRAWSCORESCALETHIRD-HIGHEST PERSONALITY SCALE BR 65 OR HIGHER: SCALE3 Inept Self-ImageInterpersonally SubmissiveImmature SCALES0607080901000060607070808090901001 00 CONFIDENTIAL INFORMATION FOR PROFESSIONAL USE ONLYN egativistic (Passive- aggressive )MCMI -III Interpretive Report ID.
8 1256611/30/2014, Page 4 Joan SampleSAMPLECOMPLETE LISTING OF MCMI-III GROSSMAN FACET SCALE SCORES1 SchizoidTemperamentally ApatheticInterpersonally UnengagedExpressively ImpassiveAvoidantInterpersonally AversiveAlienated Self-ImageVexatious RepresentationsDepressiveInept Self-ImageInterpersonally SubmissiveImmature RepresentationsHistrionicGregarious Self-ImageInterpersonally Attention-SeekingExpressively DramaticNarcissisticAdmirable Self-ImageCognitively ExpansiveInterpersonally ExploitiveAntisocialExpressively ImpulsiveActing-Out MechanismInterpersonally IrresponsibleSadisticTemperamentally HostileEruptive OrganizationPernicious RepresentationsCompulsiveCognitively ConstrictedInterpersonally RespectfulReliable Self-ImageNegativisticTemperamentally IrritableExpressively ResentfulDiscontented Self-ImageMasochisticDiscredited RepresentationsCognitively DiffidentUndeserving Self-ImageSchizotypalEstranged Self-ImageCognitively AutisticChaotic RepresentationsBorderlineTemperamentally LabileInterpersonally ParadoxicalUncertain Self-ImageParanoidCognitively MistrustfulExpressively DefensiveProjection WoefulWorthless
9 Self-ImageCognitively CLINICAL MULTIAXIAL INVENTORY - IIICONFIDENTIAL INFORMATION FOR PROFESSIONAL USE ONLYFor each of the Clinical Personality Patterns and Severe Personality Pathology scales (the scalenames shown in bold), scores on the three facet scales are shown beneath the scale -III Interpretive Report ID: 1256611/30/2014, Page 5 Joan SampleSAMPLERESPONSE TENDENCIES This patient's response style may indicate a broad tendency to magnify the level of experienced illnessor a characterological inclination to complain or to be self-pitying. On the other hand, the response stylemay convey feelings of extreme vulnerability that are associated with a current episode of acute the impetus for the response style, the patient's scale scores, particularly those on Axis I, maybe somewhat exaggerated, and the interpretation of this profile should be made with this consideration inmind.
10 The BR scores reported for this individual have been modified to account for the high self-revealinginclinations indicated by the high raw score on Scale X (Disclosure) and the psychic tension anddejection indicated by the elevations on Scale A (Anxiety) and Scale D (Dysthymia). AXIS II: PERSONALITY PATTERNS The following paragraphs refer to those enduring and pervasive personality traits that underlie thiswoman's emotional, cognitive, and interpersonal difficulties. Rather than focus on the largely transitorysymptoms that make up Axis I clinical syndromes, this section concentrates on her more habitual andmaladaptive methods of relating, behaving, thinking, and feeling.