Transcription of Measles - WHO
1 Measles Measles Last updated: October 15, 2018. vaccine -Preventable Diseases 1. WHO vaccine -Preventable Diseases Surveillance Standards Surveillance Standards Measles DISEASE AND vaccine CHARACTERISTICS. Measles is one of the most contagious diseases pneumonia, diarrhea and encephalitis can occur in up for humans. It is caused by a paramyxovirus virus, to 30% of persons depending on age and predisposing manifesting as a febrile rash illness. The incubation conditions, such as young age, malnutrition and period for Measles usually is 10 14 days (range immunocompromising conditions. These complications 7 23 days) from exposure to symptom onset (1). usually occur two to three weeks after rash onset.
2 Initial symptoms (prodrome) generally consist of Measles can infect anyone of any age, but most of the fever, malaise, cough, conjunctivitis, and coryza. The burden of disease globally is still among children < 5. characteristic maculopapular rash appears two to years of age. four days after onset of the prodrome. Patients are The Measles vaccine is a live attenuated virus vaccine ;. usually contagious from about four days before rash two doses are recommended by WHO to provide onset until four days after its appearance. The exact protection from disease. Currently, all six WHO. source of transmission is frequently unknown because regions have Measles elimination goals by or before the patient is often infected by someone in the pre- 2020, and surveillance is a key element to achieving rash prodrome stage.
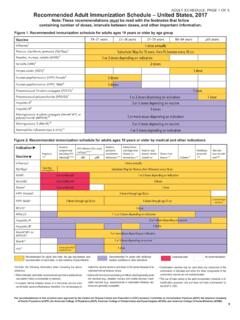
3 Measles complications such as elimination (2). FIGURE Timeline of infectivity, clinical disease and 1 laboratory findings for Measles virus infection RASH ONSET. DAYS -23 .. -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30. INFECTIVITY. Exposure period Infectious period Signs/Symptoms Prodrome Rash CLINICAL. 1-5 days 4-8 days Measles complications ( pneumonia). Measles -related death Adequate sample collection for IgM testing LAB SPECIMEN/. DIAGNOSTICS. IgM (optimal sensitivity). Viral isolation in cell culture (optimal sensitivity). RT-PCR. (optimal sensitivity). Horizontal bars represent range of possible days, with day 0 as the day of rash onset.
4 For lab specimens/. diagnostics, bars represent the range of days in which that particular test would be most likely to be positive. Virus can be detected before rash onset. Virus can be detected after day 5 but sensitivity decreases. 3. WHO vaccine -Preventable Diseases Surveillance Standards RATIONALE AND OBJECTIVES OF SURVEILLANCE. GLOBAL OR REGIONAL LEVEL The rationale for surveillance in the 2003 VPD. The key objective of Measles surveillance is to identify surveillance standards described different surveillance areas of Measles virus transmission and immunity gaps. standards for countries with different goals or at This will guide effective public health responses to different points along the Measles prevention continuum: achieve elimination of endemic Measles and sustain control, accelerated control/mortality reduction, and elimination in post-elimination settings.
5 Elimination. However, now that all regions have Measles elimination goals, all countries should strive to achieve NATIONAL OR LOCAL LEVEL elimination-standard surveillance. This document The objectives of Measles surveillance at these levels provides the standards for surveillance in countries are to: moving towards or maintaining elimination. Guidance on how to transition from surveillance in mortality- hh detect and confirm cases to ensure proper case reduction settings to elimination settings is published management and implement appropriate public elsewhere (2). health strategies to control further transmission hh investigate cases to determine the source of infection, including who infected the individual and whether the infection was imported, importation-related or BOX Integration with endemic 1 rubella surveillance hh identify populations and areas with low coverage and at higher risk of outbreaks that require enhanced Integrate Measles surveillance vaccination efforts, and determine the reason for with rubella surveillance, each Measles case: whenever possible.
6 Both diseases vaccine was recommended but person did not present as clinically similar with get it (programmatic failure) a rash illness, and both have person was vaccinated according to the regional targets of elimination. recommended schedule ( vaccine failure) As such, both should have similar approaches to surveillance. vaccine was not received because it is not Test for suspected cases of both normally recommended for this person (for Measles and rubella either in example, younger than the routine age for a parallel or in series, depending second dose of vaccine ). on local epidemiology and public hh verify the absence of endemic Measles cases to health priorities.
7 This chapter document elimination of endemic virus. specifically addresses Measles surveillance, although many details would also pertain to rubella surveillance. See the Rubella chapter for additional information about rubella. 4. Measles Measles TYPES OF SURVEILLANCE RECOMMENDED. MINIMAL SURVEILLANCE public), with a system for zero reporting (reporting In elimination mode, Measles surveillance must be that there were no cases). If desired and resources exist, case-based. The surveillance system should be able consider implementing community-based surveillance to do the following in a timely manner: detect, notify (such as notification of cases by community health and investigate suspected Measles cases and outbreaks; workers or teachers) in areas that are at risk for Measles , correctly classify cases as confirmed or discarded; during outbreaks, and in populations where not all determine if they were due to failure of programme Measles cases seek care in health facilities.
8 Implementation (for example, should have been vaccinated but were not), due to vaccine failure, or occur LINKAGES TO OTHER SURVEILLANCE. in someone for whom vaccination is not recommended; Surveillance for Measles should be done together with and inform actions that reduce morbidity and mortality rubella (see Box 1). Also consider integrating other and prevent further virus transmission (2). rash-causing diseases such as dengue into this Active surveillance in health facilities, such as regular surveillance system, given the broad case detection review of clinic logbooks for missed cares, is essential so definition for Measles . no cases are missed. Surveillance should be nationwide with inclusion of all health facilities (both private and CASE DEFINITIONS AND FINAL CLASSIFICATION.)
9 SUSPECTED CASE DEFINITION FOR CASE FINDING hh Epidemiologically linked Measles : A suspected A suspected case is one in which a patient with fever case of Measles that has not been confirmed by a and maculopapular (non-vesicular) rash, or in whom a laboratory, but was geographically and temporally health-care worker suspects Measles . related with dates of rash onset occurring 7 23 days apart from a laboratory-confirmed case or another FINAL CASE CLASSIFICATION epidemiologically linked Measles case. hh Laboratory-confirmed Measles : A suspected case of hh Clinically compatible Measles : A suspected case Measles that has been confirmed positive by testing with fever and maculopapular (non-vesicular) rash in a proficient laboratory, and vaccine -associated and at least one of cough, coryza or conjunctivitis, illness has been ruled out (see the section below, but no adequate clinical specimen was taken and Other definitions for Measles cases).
10 A proficient the case has not been linked epidemiologically to laboratory is one that is WHO-accredited or a laboratory-confirmed case of Measles or other has established a recognized quality assurance communicable disease. As countries get closer programme, such as International Organization to elimination, the vast majority of Measles for Standards (ISO) or Clinical Laboratory cases should be confirmed by laboratory or Improvement Amendments (CLIA) certification (3). epidemiological linkage. Clinically compatible cases are highly unlikely to be Measles when the country is at or near elimination. 5. WHO vaccine -Preventable Diseases Surveillance Standards hh Non- Measles discarded case: A suspected case that confirmation of another etiology has been investigated and discarded as a non- Measles failure to meet the clinically compatible Measles (and non-rubella) when any of the following are case definition.