Example: bankruptcy
Medical Referral Form
Loss of Consciousness Uncontrollable Diabetes Dementia/Memory Deficits . Psychiatric Disturbance Drug/Alcohol Addiction Severe Visual Deficit . Sleep Disorder Other . Please explain each area that was marked: Please indicate how you know this individual (friend, family member, patient, etc.):_____
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

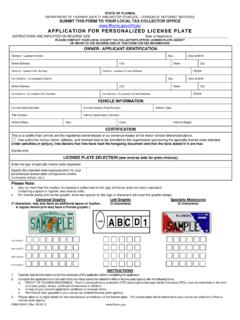
APPLICATION FOR PERSONALIZED LICENSE PLATE
www.flhsmv.govstate of florida department of highway safety and motor vehicles – division of motorist services submit this form to your local tax collector office
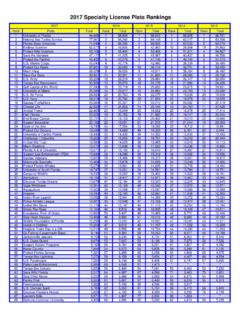
2017 Specialty License Plate Rankings
www.flhsmv.gov2017 Specialty License Plate Rankings Rank Plate Total Rank Total Rank Total Rank Total Rank Total 1 University of Florida 94,685 1 88,906 1 96,643 1 88,805 1 96,701
APPLICATION FOR PERSONALIZED LICENSE PLATE
www.flhsmv.govstate of florida department of highway safety and motor vehicles – division of motorist services submit this form to your local tax collector office
2017 Specialty License Plate Rankings
www.flhsmv.gov2017 Specialty License Plate Rankings Rank Plate Total Rank Total Rank Total Rank Total Rank Total 1 University of Florida 94,685 1 88,906 1 96,643 1 88,805 1 96,701

STATE OF FLORIDA DEPARTMENT OF HIGHWAY …
www.flhsmv.govstate of florida department of highway safety and motor vehicles – division of motorist services submit this form to your local tax collector office

STATE OF FLORIDA Department of Highway Safety …
www.flhsmv.govSTATE OF FLORIDA Department of Highway Safety and Motor Vehicles APPENDIX " C "Uniform Traffic Citation Manual 316.0741 HIGH OCCUPANCY VEHICLE LANES

APPENDIX C 2012 Revision - Florida Department of …
www.flhsmv.govSTATE OF FLORIDA Department of Highway Safety and Motor Vehicles APPENDIX " C "316.074(1) TRAFFIC CONTROL DEVICE …

PUBLIC OFFICIAL, LAW ENFORCEMENT AGENCY …
www.flhsmv.govpublic official, law enforcement agency personnel and others pursuant to section 119.071, florida statutes request to withhold personal information
Department of Highway Safety and Motor Vehicles
www.flhsmv.govDepartment of Highway Safety and Motor Vehicles . Electronic Lien and Title Program . Lienholder’s Guide. This guide provides lienholders with the necessary information to participate in the

FLORIDA DEPARTMENT OF HIGHWAY SAFETY …
www.flhsmv.govflorida department of highway safety and motor vehicles application for disabled person parking permit *****submit application to your local county tax collector's office or license plate agency*****
Related documents
Understanding Alzheimer's and Dementia
alz.orgVascular dementia is the second most common cause of dementia after Alzheimer’s disease. » Dementia with Lewy bodies is a type of progressive dementia related to buildup of a protein called alpha-synuclein that damages brain cells. Early symptoms include hallucinations and sleep problems. » Frontotemporal dementia (FTD) is a group of disorders.
ACTIVITY IDEAS FOR ALZHEIMER’S/DEMENTIA RESIDENTS
www.nccdp.orgALZHEIMER’S/DEMENTIA RESIDENTS Activity Ideas There are many different stages that a person with Alzheimer's and Dementia will go through. It is ... Exercise will aide in helping a person to sleep. A stroll in the wheelchair is great exercise, if the person is …
LEWY BODY DEMENTIA - National Institutes of Health
order.nia.nih.govdementia, cognitive symptoms develop more than a year after the onset of movement problems. Not-so-sweet dreams In his mid-60s, Bruce started having mild confusion and vivid dreams in which he thrashed around and even fell out of bed . His neurologist diagnosed REM sleep behavior disorder and mild cognitive changes . Two years later, Bruce’s

GERIATRIC FUNCTIONAL ASSESSMENT
www.med.umich.edudementia) who: • Are age 80 years or above • Are undergoing elective surgery • Have recently been discharged from the hospital • Undergo unexplained decline in functional status • Have unexplained sleep difficulties or behavioral disturbances • Have poor adherence with medical or behavioral regimens

ICF Checklist revSep2003 - WHO
www.who.intb117 Intellectual ( incl. Retardation, dementia) b130 Energy and drive functions b134 Sleep b140 Attention b144 Memory b152 Emotional functions b156 Perceptual functions b164 Higher level cognitive functions b167 Language b2. SENSORY FUNCTIONS AND PAIN b210 Seeing b230 Hearing b235 Vestibular (incl. Balance functions) b280 Pain b3. VOICE AND ...

Statistical - Postpartum
www.postpartum.netdementia, dipsomania, and epilepsy. In 1917 the Census Bureau, ... sleep disturbance, psychomotor agitation or retardation, decreased energy, feelings of worthlessness or guilt, difficulty concentrating or thinking, and thoughts of death or suicide or suicidal attempts.

Mall Walking: A Program Resource Guide
www.cdc.govweight, improving sleep, and for older adults, maintaining their independence, reducing their risk of falls, and delaying the onset of cognitive decline and dementia (Physical Activity Guidelines Advisory Committee, 2008). To gain health beneits, national guidelines recommend that adults, including older adults,

Intro to Dementia slide handouts - Florida
apd.myflorida.com6/9/2010 1 Vascular Dementia • Accounts for about 20% of dementia • Can come from a series of strokes in large and small vessels. (anoxia) • Prevention is the key:
Life Plan for the Life Span
www.apa.orgnutritious diet, adequate sleep, and regular physical activity. • See your health-care provider for recommended preventive health services. • Develop skills to manage stress and regulate your emotional health. • Educate yourself about health, self-care, and • •
NTG-EDSD - aadmd.org
aadmd.orgNTG-EDSD - page 3 [Check column option as appropriate] Always been the case but worse New symptom in past year Does not apply (19)Activities of Daily Living Needs help …