Transcription of Proof of medical exemption
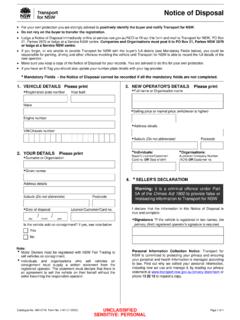
1 Proof of medical exemption People aged 16 or over now need to show Proof of COVID-19 vaccination or a signed medical exemption as a condition of entry to most businesses. Here's what's accepted as Proof of medical exemption : COVID-19 medical clearance notice COVID-19 medical exemption form COVID-19 VACCINE medical COVID-19 VACCINE medical . medical Clearance Notice medical Clearance Notice CONTRAINDICATION CONTRAINDICATION. Under Public Health (COVID-19 Self-Isolation) Order (No 3) 2021 [NSW] Under Public Health (COVID-19 Self-Isolation) Order (No 3) 2021 [NSW]. To whom it may concern, To whom it may concern, I am a registered medical practitioner.
2 I certify that, Given name: I am a registered medical practitioner. I certify that, Given name: Family name: DOB: / / Sex: Male Female Prefer not to say Family name: DOB: / / Sex: Male Female Prefer not to say To Whom It May Concern, To Whom It May Concern, Residential address: Residential address: CITIZEN, Jane DOB: 12-01-1956 of 10 City St, Suburb, 2000 was required to self-isolate CITIZEN, Jane DOB: 12-01-1956 of 10 City St, Suburb, 2000 was required to self-isolate Section A medical contraindication Section A medical contraindication 1 1. under the Public Health (COVID-19 Self-Isolation) Order (No 3) 2000 [NSW], or an order under the Public Health (COVID-19 Self-Isolation) Order (No 3) 2000 [NSW], or an order Has the following medical contraindication(s) to receiving a dose of all of the COVID-19 vaccines available for use in Australia: Has the following medical contraindication(s) to receiving a dose of all of the COVID-19 vaccines available for use in Australia: that remakes that order, (the Order) to prevent transmission of COVID-19.
3 That remakes that order, (the Order) to prevent transmission of COVID-19. Pfizer (Comirnaty) Moderna (Spikevax). AstraZeneca (Vaxzevria) COVID-19 vaccine Pfizer (Comirnaty) Moderna (Spikevax). AstraZeneca (Vaxzevria) COVID-19 vaccine COVID-19 vaccine COVID-19 vaccine COVID-19 vaccine COVID-19 vaccine This notice confirms CITIZEN, Jane has been assessed under that Order as no longer This notice confirms CITIZEN, Jane has been assessed under that Order as no longer Dose 1 Dose 2 Dose 1 Dose 2 Dose 1 Dose 2 Dose 1 Dose 2 Dose 1 Dose 2 Dose 1 Dose 2. infectious for COVID-19 and is medically cleared under the Order. infectious for COVID-19 and is medically cleared under the Order.
4 History of anaphylaxis History of anaphylaxis to a component of the AstraZeneca History of anaphylaxis History of anaphylaxis to a component of the AstraZeneca History of anaphylaxis History of anaphylaxis to a component of the to a component of the (Vaxzevria) COVID-19 vaccine to a component of the to a component of the (Vaxzevria) COVID-19 vaccine As CITIZEN, Jane has been medically cleared from COVID-19, for 6 months from the As CITIZEN, Jane has been medically cleared from COVID-19, for 6 months from the Pfizer (Comirnaty) Moderna (Spikevax) History of capillary leak syndrome Pfizer (Comirnaty) Moderna (Spikevax) History of capillary leak syndrome date of this notice in NSW they: date of this notice in NSW they: COVID-19 vaccine COVID-19 vaccine COVID-19 vaccine COVID-19 vaccine History of any of the following medical conditions: History of any of the following medical conditions: Serious adverse event Serious adverse event cerebral venous sinus thrombosis (CVST) Serious adverse event Serious adverse event cerebral venous sinus thrombosis (CVST).
5 Are taken, under any NSW public health order to be fully vaccinated, are taken, under any NSW public health order to be fully vaccinated, attributed to the first dose attributed to the first dose attributed to the first dose heparin - induced thrombocytopenia (HIT) attributed to the first dose heparin - induced thrombocytopenia (HIT). of the Pfizer (Comirnaty) of the Moderna (Spikevax) of the Pfizer (Comirnaty) of the Moderna (Spikevax). SAMPLE ONLY SAMPLE ONLY. idiopathic splanchnic (mesenteric, portal or splenic) idiopathic splanchnic (mesenteric, portal or splenic). are taken, under any NSW public health order to have met any testing requirements are taken, under any NSW public health order to have met any testing requirements COVID-19 vaccine, being: COVID-19 vaccine, being: COVID-19 vaccine, being: COVID-19 vaccine, being: SAMPLE ONLY SAMPLE ONLY.
6 Vein thrombosis vein thrombosis antiphospholipid syndrome (APLS) with thrombosis antiphospholipid syndrome (APLS) with thrombosis will not need to self-isolate as a close contact of COVID-19 case will not need to self-isolate as a close contact of COVID-19 case Other specified medical and/or miscarriage Other specified medical and/or miscarriage Other specified medical Other specified medical contraindication, being: Serious adverse event attributed to the first dose of the contraindication, being: Serious adverse event attributed to the first dose of the However, if CITIZEN, Jane is subject to a direction under a NSW Public Health Order However, if CITIZEN, Jane is subject to a direction under a NSW Public Health Order contraindication, being: AstraZeneca (Vaxzevria) COVID-19 vaccine, being: contraindication, being: AstraZeneca (Vaxzevria) COVID-19 vaccine, being: requiring a person to show their vaccination evidence or testing documentation to certain requiring a person to show their vaccination evidence or testing documentation to certain SAMPLE.
7 Persons, such as NSW Police, NSW Health, the occupier of the premises or the person's persons, such as NSW Police, NSW Health, the occupier of the premises or the person's Other specified medical contraindication, being: Other specified medical contraindication, being: employer, this notice must be produced on request. employer, this notice must be produced on request. For further details, about this medical clearance notice see For further details, about this medical clearance notice see ONLY. OR OR. 2 2. Section B Temporary medical contraindication for up to 6 months Section B Temporary medical contraindication for up to 6 months Yours sincerely Yours sincerely Has the following temporary medical contraindication(s) to receiving dose 1 dose 2 of any of the COVID-19 vaccines Has the following temporary medical contraindication(s) to receiving dose 1 dose 2 of any of the COVID-19 vaccines available for use in Australia until / / (up to 6 months) available for use in Australia until / / (up to 6 months).
8 CITIZEN, David CITIZEN, David acute major illness, being: acute major illness, being: medical Practitioner medical Practitioner significant immunocompromise of short duration, being: significant immunocompromise of short duration, being: 3. past confirmed infection with SARS-CoV-2 within the last 6 months . Date of diagnosis: / / 3. past confirmed infection with SARS-CoV-2 within the last 6 months . Date of diagnosis: / /. DATE: 01-10-2021 12:27 DATE: 01-10-2021 12:27. other specified temporary medical contraindication, being: other specified temporary medical contraindication, being: medical practitioner details medical practitioner details Name: Telephone: Name: Telephone: Address: Email: Address: Email: Registration Registration Number: M E D 0 0 0 Number: M E D 0 0 0.
9 Signature: Date: Signature: Date: Confidential Confidential Print and Sign / / Print and Sign / /. NH700729A 15 September 2021 NSW Ministry of Health. NH700729A 15 September 2021 NSW Ministry of Health. ORIGINAL: NSW HEALTH RECORDS COPY: TO PATIENT 1/2 ORIGINAL: NSW HEALTH RECORDS COPY: TO PATIENT 1/2. (Shown as a digtal pdf) (Shown as colour print) (Shown as black & white print) (Shown as colour print. (Shown as black & white print. Must be signed by a doctor) Must be signed by a doctor). COVID-19 digital certificate - medical exemption Certificate validation SAMPLE. ONLY SAMPLE ONLY SAMPLE ONLY. (Shown on a Medicare online (Shown as colour print.))
10 (Shown as black & white print. (Shown on the Service NSW app account through myGov) Must be signed by a doctor) Must be signed by a doctor) available from 17 October). Immunisation history statement - medical exemption Immunisation history statement Immunisation history statement As at: 21 September 2021 As at: 21 September 2021. For: JOHN CITIZEN For: JOHN CITIZEN. Date of birth: 01 January 1950 Date of birth: 01 January 1950. Individual Healthcare Identifier (IHI): 8003 60XX XXXX XXXX Individual Healthcare Identifier (IHI): 8003 60XX XXXX XXXX. Date given Immunisation Brand name given Date given Immunisation Brand name given 01 Sep 2021 COVID-19 Pfizer Comirnaty 01 Sep 2021 COVID-19 Pfizer Comirnaty Next NIP immunisation/s due Date due Next NIP immunisation/s due Date due No vaccines due.