Transcription of SECONDARY WOUND CLOSURE - Practical Plastic Surgery
1 SSEECCOONNDDAARRYY WWOOUUNNDD CCLLOOSSUURREES econdary WOUND CLOSURE is also referred to as CLOSURE by secondaryintention. The skin edges of the WOUND are not sutured together; thewound is left open. Dressings are applied regularly to keep thewound clean, and the WOUND gradually closes and heals on its WOUND CLOSURE requires little technical expertise. It is thesimplest and, therefore, lowest rung on the reconstructive ladder. This chapter discusses the important background knowledge you musthave when deciding to allow SECONDARY WOUND it is often true that the easiest treatment is the one to choose,you must be aware of what SECONDARY WOUND CLOSURE involves fromthe patient s Healing PeriodIt may take several weeks to even months for the WOUND to heal usingdressings alone. This extended healing period can cause considerablehardship for the patient. From a financial standpoint, the patient maynot be able to return to work with the open WOUND .
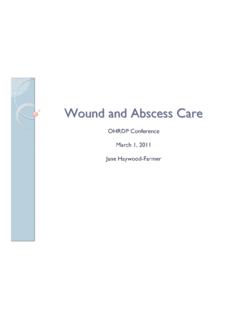
2 In addition, dress-ing supplies, no matter how simple you make them, can get LocationThe location of the WOUND may make it impossible for the patient tochange the dressings. For example, the patient will require outside as-sistance to care for a WOUND on the back or the buttocks. It also may bedifficult to keep the dressings in place during treatment of a 10 KKEEYY FFIIGGUURREE::Dead space under skin closure86 Practical Plastic Surgery for NonsurgeonsPainThe sensation associated with an open WOUND can range from some-what bothersome to quite painful. Dressing changes are often painfulas well. Some pain medications are addictive when given for the longperiod required for a large WOUND to that are allowed to heal secondarily tend to have larger andmore noticeablescars than the scars that results from primary healing also has a greater tendency for hypertrophicscar/keloid formation, which can be bothersome and unsightly.
3 Scar tightness and contracturecan be especially problematic in areassuch as the upper cheek, where a tight scar can pull down and distortthe lower eyelid, or in the arm pit (axilla), where scar problems canlead to limited shoulder mobility and WOUND that heals secondarily has a less stablescar that is, the scaris more easily injured than the scar from a WOUND with primary clo-sure. Over the years less stable scars may be chronically injured. Theymay reheal only to be reinjured again and again. This cycle can be quitetroublesome and also is associated with a risk for the development ofan aggressive skin SSeettttiinnggss ffoorr SSeeccoonnddaarryy CClloossuurreeWounds that will heal with an acceptable scar if the skin edges are notsutured together can be allowed to heal secondarily. Examples include: Relatively small smaller than 11 2cm often healquite well by SECONDARY intention.
4 Even wounds with a diameter of3 4 cm or larger, with no exposed tendons, bones, or other importantstructures, can be allowed to heal secondarily when lack of surgicalexpertise allows no other option. Be sure to keep in mind the abovecaveats when wounds > 2 cm are allowed to close by SECONDARY in-tention. Second-degree burns are often allowed to healwith local WOUND care alone. See chapter 20, Burns, for a morethorough CClloossuurree aass tthhee TTrreeaattmmeenntt ooff CChhooiicceeSome wounds should notbe closed with sutures. Instead, they shouldbe left open and treated with dressing changes until they include: SECONDARY WOUND CLOSURE 87 Wounds that come to your attention more than 6 hours after the exception of facial wounds, you should not use pri-mary repair for a WOUND that is more than 6 hours old. The risk ofinfection is greatly increased after this amount of time has lapsed.
5 Highly contaminated dirty WOUND should not be closedbecause of concerns about WOUND infection. Examples of dirtywounds include human bites on the hand or wounds deeply embed-ded with dirt or grass. Wounds with dead space under the skin emptyspace rather than subcutaneous tissue is seen beneath the repairedskin when you try to bring the skin edges together. This dead spaceoccurs due to loss of subcutaneous tissue or swelling of the skinaround the WOUND . If such wounds are closed primarily, the risk forblood collecting under the skin CLOSURE is high, increasing the likeli-hood of infection and problems with WOUND healing. Wounds with too much swelling or skin swelling orskin loss makes the skin CLOSURE very tight. A tight skin CLOSURE de-creases blood circulation to the skin edges, thereby causing the tis-sues to become ischemic (low supply of oxygen and nutrients).
6 If thetightness does not soon resolve, the skin may die. Skin death resultsin a WOUND that is larger than the initial WOUND and even more prob-lematic to the skin is sutured together, the underlying tissues are not well approxi-mated. This dead space promotes hematoma (a collection of old blood) forma-tion and Practical Plastic Surgery for NonsurgeonsCCoonnttrraaiinnddiiccaattiio onnss ttoo SSeeccoonnddaarryy CClloossuurreeCertain wounds should not be allowed to heal by SECONDARY are wounds that are associated with exposure of an importantunderlying structure or are located in areas where a tight scar will beparticularly problematic. Such wounds should be closed primarily. Ifprimary CLOSURE is not possible, one of the other options from the re-constructive ladder must be chosen (see following chapters).Exposure of a Vital StructureSometimes wounds occur over important structures such as fracturesites, tendons, or prosthetic devices ( , artificial joints).
7 If these struc-tures are not covered by healthy soft tissue, there is an almost 100%risk for the structure to become infected or avoid permanent disability, a WOUND that results in exposure of animportant structure should optimally be closed quickly (within days)with healthy Where a Tight Scar is UndesirableWounds over CreasesSecondary CLOSURE is not useful on wounds that are larger than 3 4 cmand located over creases ( , front of the elbow [antecubital fossa],armpit [axilla]). The scar that results from SECONDARY CLOSURE will causetightness across the crease and may result in significant limitation ofmovement. If splints and movement exercises are used diligently (seechapter 15, Scar Formation ), this problem may be avoided. But evenwith the best of care, limitation of movement often Wounds Near the Lower EyelidIn many areas of the face, a WOUND can be allowed to heal secondarilywithout significant cosmetic ill effects.
8 However, wounds on the cheeknear the lower eyelid may pull the eyelid downward if allowed to healsecondarily. The result not only is cosmetically unacceptable but alsomay expose the eye to ffoorr UUssee ooff SSeeccoonnddaarryy CClloossuurreeIf you decide to treat a WOUND by SECONDARY intention, the WOUND mustbe evaluated thoroughly and cleaned rigorously. The appropriatedressing regimen must then be implemented. See chapter 9, TakingCare of Wounds, for specific dressing WOUND CLOSURE 89 Unless the WOUND involves a human or a deep animal bite, antibiotics(oral or intravenous) are not required. However, you should see the pa-tient within a few days to ensure that no signs of infection are presentand that the WOUND is being cared for of InfectionSigns of WOUND infection include redness, warmth, swelling, and ten-derness in the tissues around the WOUND . Drainage of pus from thewound is also a sign of exudate on top of the WOUND does notmean that the WOUND is in-fected.
9 It is often just proteinaceous debris from the WOUND itself. Agreen, somewhat sweet-smelling, creamy material is a sign of coloniza-tion by Pseudomonasbacteria. Without signs of surrounding soft tissueinfection, antibiotics are not required. However, you should treat thewound with wet-to-dry dressing changes, preferably with Dakin s so-lution, and increase the number of changes each in Dressing RegimenDo notbe afraid to change dressing regimens. You may start with adressing regimen of antibiotic ointment covered with dry gauze. Aftera few days, a lot of exudate covers the WOUND . At this point you shouldchange to a wet-to-dry dressing and observe how the WOUND pro-gresses. Once the WOUND has improved in appearance, you can go backto the antibiotic ointment or continue with the wet-to-dry of WOUND DressingThe dressings should be continued until the WOUND heals. Oftenduring the course of SECONDARY healing, the WOUND develops a dryeschar (scab).
10 The patient can cover the area with dry gauze or evenleave it uncovered. As the WOUND heals, the eschar gradually falls the WOUND is near a crease, encourage the patient to exercise the areato prevent formation of a tight scar. Splints also may be useful. Seechapter 15, Scar Formation, for more Goldwyn RM, Rueckert F: The value of healing by SECONDARY intention for sizable de-fects of the face. Arch Surg 112:285, Montandon D, D Andiron G, Gabbiani G: The mechanism of WOUND contraction andepithelialization. Clin Plast Surg 4:325, 1977.