Transcription of Surgical Technique - Stryker MedEd
1 MDM X3 Modular Dual Mobility acetabular SystemSurgical TechniqueOrthopaedicsInDIcatIOnsThe indications for use of total hip replacement prostheses include: Non-inflammatory degenerative joint disease including osteoarthritis and avascular necrosis. Rheumatoid arthritis. Correction of functional deformity. Revision procedures where other treatments or devices have failed. Treatment of non-union, femoral neck and trochanteric fractures of the proximal femur with head involvement that are unmanageable using other techniques. Dislocation risks.*The Modular Dual Mobility (MDM) Liner is intended for cementless use Overt infection. Distant foci of infections (which may cause hematogenous spread to the implant site). Rapid disease progression as manifested by joint destruction or bone resorption apparent on roentgenogram. Skeletally immature patients.
2 Cases where there is a loss of abductor musculature, poor bone stock or poor skin coverage around the hip joint which would make the procedure presentIng IncreaseD rIsk Of faIlure: Uncooperative patient or patient with neurologic disorders, incapable of following instructions; Osteoporosis; Metabolic disorders which may impair bone formation; or, anD precautIOnsSee package insert for warnings, precautions, adverse effects and other essential product information. The MDM Liner is intended for use with Trident or Tritanium acetabular cups only. Additionally, the MDM Liner is not intended for use as a metal-on-metal or ceramic-on-metal articulation. No testing has been conducted to determine that these bearing couples produce favorable mechanical outcomes. Only Stryker or 28mm femoral heads should be inserted into the ADM/MDM polyethylene inserts.
3 Further, do not substitute another manufacturer s device for any component of the ADM/MDM acetabular System. Any such use will negate the responsibility of Howmedica Osteonics Corp. for the performance of the resulting mixed component implant. Before using MDM instrumentation, verify: Instruments have been properly disassembled prior to cleaning and sterilization; Instruments have been properly assembled post-sterilization; Instruments have maintained design integrity; and, Proper size configurations are Of cOntentsPre-operative Planning and X-ray Evaluation ..2 acetabular Preparation ..3 Spherical Reaming ..4-5 Final Reaming ..6 Trial Evaluation ..7 Shell Implantation ..8-9 Optional Screw Utilization ..10-11 Trial Insert Reduction ..12 Liner Implantation ..12-13 Trial Insert/Head Reduction ..14-16 Insert/Head Implantation ..17 Reduction and Closure.
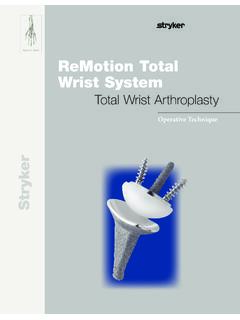
4 18 Removal Options ..19 Catalog Information ..20-23 MDM X3 DesIgn ratIOnale The MDM System incorporates the following dual points of articulation: or 28mm femoral head; and, Large polyethylene insert that mimics a femoral shellMDM cocr linerpoly Insertfemoral Headtable 1: MDM Liner and Insert Compatibility with Trident and Tritanium ShellsT his publication sets forth detailed recommended procedures for using Stryker Orthopaedics devices and instruments. It offers guidance that you should heed, but, as with any such technical guide, each surgeon must consider the particular needs of each patient and make appropriate adjustments when and as Dual Mobility acetabular SystemIntrODuctIOnsHell sIze (mm), lIner alpHa cODeTrident PSL Shell4446, 4850, 5254, 5658, 60 62, 6466, 6870, 72 Trident Hemispherical Shell4648, 5052, 5456, 5860, 6264, 6668, 7072, 74 Tritanium Hemispherical Shell4850, 5254, 5658, 6062, 6466, 6870, 7274-80 Liner Alpha CodeCDEFGHIJMDM CoCr Liner36C38D42E46F48G52H54I58 JPoly Insert OD (mm)3638424648525458 Poly Insert ID (mm) Poly Thickness (mm) 12 MDMX3 Surgical tecHnIquepre-OperatIve plannIng anD X-ray evaluatIOn Pre-operative planning and X-ray evaluation aids in the selection of the most favorable implant design and optimal size for the patient s hip pathology.
5 Pre-operatively selecting potential implant designs and sizes can facilitate operating room preparation and assure availability of appropriate sizes. X-ray evaluation may also help detect anatomic anomalies that could prevent the intra-operative achievement of the established pre-operative 2 3acetabular preparatIOnThe acetabulum is prepared by the release and removal of soft tissue using the surgeon s preferred Technique to gain adequate exposure for reaming. Excision of the labrum and osteophytes allows for proper visualization of the bony anatomy and improves ease of Orthopaedics Femoral and Wing Retractors can be utilized to gain acetabular exposure (Figure 1). With the acetabulum exposed, bony defects can be identified. If necessary, bone grafting options may be 1careful identification and removal of osteophytes can help reduce the possibility of bone-to-bone or component-to-bone impingement.
6 Additionally, this can aid in the identification of bony landmarks used for cup 3aIt is recommended that the initial reaming begin with a CuttingEdge Spherical Reamer that is 4mm smaller than the templated or gauged size. The reamer is attached to the reamer handle by pushing down on the reamer and applying a quarter-turn to lock in place. Reaming progresses in 1mm increments until final sizing is achieved. Surgical judgment is used to assess bone stock, amount of interference, adequacy of medialization and proper amount of reaming as desired. spHerIcal reaMIngall external alignment guides depend on knowing that the patient is in a lateral decubitus position and that there is no pelvic in pelvic tilt and pelvic flexion caused by patient positioning on the table, as well as disease in contralateral hip, spine and pelvis may impact a surgeon s ability to achieve component placement of 45 /20 abduction/anteversion.
7 NOteWilliam a. leone, Jr., t o achieve the recommended 45 abduction and 20 anteversion, an optional pelvic alignment level (pal) may be used. for recommended Technique , refer to the pal Surgical protocol, lsp61. John andronaco, be sure to check for and remove internal osteophytes prior to reaming for the implant to prevent lateralizing the shell. tIpsTo obtain optimal component positioning in the reaming process, a 45 /20 Abduction/Anteversion Alignment Guide can be attached to the CuttingEdge Reamer Handle (Figure 2). The alignment guide, when perpendicular to the long axis of the patient, will orient the reamer handle at 45 of abduction, thereby placing the axis of the spherical reamer at 45 of inclination (Figure 3). The reamer handle may be positioned at 20 of anteversion by aligning the left/right anteversion rod on the alignment guide so that it is parallel to the long axis of the the cuttingedge spherical reamers should be used to prepare the acetabulum for the trident or tritanium acetabular shell 2 Figure 34 MDMX3 Surgical tecHnIque45 5 William capello, pay special attention to differential bone densities that could cause eccentric reaming.
8 TIpFigure 4the cuttingedge spherical reamers are very aggressive and perform best when sharp. care should be taken to protect the reamer from unnecessary handling, as dull or damaged cutting teeth may cause improper reaming. Dull cutting teeth will deflect to cut softer bone and resist hard bone. this situation may result in an irregularly shaped or enlarged acetabulum full profile of the CuttingEdge Spherical Reamer necessitates reaming to the full depth. The reamer head should be driven to the point where the rim/cross bar contacts the acetabular wall at the peripheral lunate region. Removal of the reamer from the handle is performed by pulling back on the locking sleeve and rotating the reamer head a quarter-turn in a clockwise direction (Figure 4).Care should be taken so as not to enlarge or distort the acetabulum by eccentric reaming.
9 Final acetabular reaming ideally shows the hemispherical acetabulum denuded of cartilage, with the subchondral plate preferably intact, and the acetabular walls preserved. locking sleevestep 3b6 MDMX3 Surgical tecHnIquefInal reaMIngtritanium solid back, cluster and Multi-Hole shell: Full Surgical Technique details for Tritanium Solid Back and Cluster Hole Shells can be found in LSP66. Full Surgical Technique details for Tritanium Multi-Hole Shells can be found in implanting the Tritanium Solid Back, Cluster Hole, or Multi-Hole Shell, it is recommended to under-ream by 1mm. As with all manufacturing processes, due to the nature of the coating, the outer diameter may be slightly larger than the size indicated. The surgeon should consider this during acetabular preparation. Depending on acetabular bone quality, the surgeon may choose to ream Hemispherical: Full Surgical Technique details can be found in by 1 to 2 mm of the actual Trident Hemispherical shell size is recommended to achieve interference psl: Full Surgical Technique details can be found in Trident PSL HA shell periphery is larger than the stated size ( , 52mm shell = periphery at the rim of the shell).
10 The size of the Trident PSL HA shell selected should be the same as the largest diameter of the CuttingEdge Spherical Reamer used. Surgical judgment is used to assess bone stock, amount of interference and proper amount of reaming as desired. When implanting the Trident PSL HA shell, the of interference fit is not always necessary when dense, hard, sclerotic bone is amount of interference fit for trident and tritanium acetabular shells should be determined intraoperatively based upon the patient s bone Izant, assess patient bone quality prior to implantation. If patient possesses hard, type a bone, line-to-line reaming is recommended. If proper bone quality exists, it is advised to under-ream by 1mm. tIpsWhen osteoporotic bone is encountered, it is recommended to under-ream by 1mm. When sclerotic bone is encountered, it may be difficult to fully seat the shell with a 1mm interference fit.