Transcription of Treatment of Diphenhydramine Cardiac Toxicity …
1 Treatment of Diphenhydramine CardiacToxicity lmplicationof Treatment withPhenytoin: of Type1aAntiarrhythmicToxicity MichaelB. Gutman, Abstract MD, PhD,FRCPC, Case Report: A 30 year old female ingesteda lar-ueanlount of Diphenhydramine . S h o rtl y a fte r. she exhi bi tedsei zureacti vi ty and w i de-conrpl extachyca r dia. Seizur e FACEP. a c ti v i ty w a s successful l ytreatedw i th i ntravenousbenzodi azepi nes and or ot r acheal Departmentof . i d e - c o m p l e xt a c h y c a r d i ai n i t i a l l y r e s o l v e du ' i t h i n t r a v e n o u s o d i u m i n t u b a t i o nW. Traumatologyand b i c a r b o n a t eb u t l a t e r r e c u r r e dd e s p i t ea l k a l i n i z a t i o nt o a p H o f 7 . 5 2 a n d a r t e r i a l Emergency Medicine, pCO,28 mmHg.
2 The wide complextachycardiaresolvedshortlyafier the intravenous University of Connecticut, Hartford. CT,USA infusionof phenytoin750 mg. Drug screeningfor tricyclic overdoseas well as other common toxic ingestantswas n e g a ti v e . RobertNoseworthy, Conclusion:Phenytoinrnay havehad therapeuticvaluein this caseof cardiactoxicity MD,FRCPC from Diphenhydramine that was refractoryto alkalinizationwith sodiumbicarbonate. Departmentof Emergency Medicine, Royal Columbian lntroduction Hospital, NewWest Diphenhydramine ingestionresultingin Toxicity has beenreportedvery commonly( l). Minister, BC,Canada Thereis someevidenceto suggest that the cardiotoxicityof diphenhydramineis similarto tricyclicanti-depressant (TCA) thatit hastype la antiarrhythmic properties (2).
3 Roy Pursell,MD, We will presenta casein which the usualmodalitiesfbr type la antiamhythmic Toxicity FRCPC,FACEP were unsuccessful in treatinga Diphenhydramine cardiotoxicitybut Department ofSurgery, w i l l th e n re vi ew the l i teratureand di scussthe use of phenytoi ni n treat ingt ype la Division of Emergency antiarrhythmic Toxicity . Medicine, andBritish ColumbiaPoison Center, CaseStudy of British University Columbia,Vancouver, BC, The 30 year old Koreanf' her boyfriendlyin-ebesideher with Canada noisy eyeswere open but she was not respondingto touch or v o i c e . S h e had l ast been seen aw ake and w el l one hour before. The pat ient had atternptedsuicidewith Sominex,,,, ( Diphenhydramine ) one month patient had no othermedicalproblemsand asidefrom Sominex,u, was on no medication.
4 On e h o u r a nd fi fteen rni nutesafter l ast bei ng seen w el l the pati entbe ganhaving generalizedseizureslastingat leastthirty five treatedthe patient AddressforCorrespondence: pre-hospital with Valium,",20 mg IV, midazolam5 mg IV and endotracheal intubation. MichaelGutman, MD,PhD, They alsoadministered100ml of D50W IV, eventhougha chemstrip,.showednormal FRCPC, FACEP. Departmentof Emergency fingerstickglucoserange,thiamin50 mg and mg IV. Hospital Initially when the paramedicsarrivedand were beginningto treat the sinus andMedicalCenter ta c h y c a rd i aat a rate of 120 w as noted on the cardi acmoni syst olicblood 114 Woodland Street pressurewas 120 mmHg. As the seizureprogressedthe QRS complex was noted to Hartford, CT06105 USA w i d e n.
5 An onl i ne order w as gi ven to admi ni sterN aH C O3 88 meq. IV. The Q RS. Tel:+(860). 714-4017 narrowedshortly thereafter. Fax:+(860)714-8046. The paramedicsarrived with the patientto the emergencydepartment(ED) 45 minutes E-mail: mgut afterthe first patientcontactat the that time, in the ED, the oxygensaturation w a s I O O % .g l u c o m e t esr h o w e ds e r u mg l u c o s ea t l l m m o l / l ( 1 9 8 m g / d l ) ;p u l s e 130/minwide complex;blood pressurell0/70: ventilated@ l6lmin. Her temperature w a s 3 8 .8 " C .The pati ent' sw ei ght w as approxi matel y50 K g. H er neck was supple. There were no signsof heador neck was good air entry heart soundswere normal with good abdomenwas soft and no lsraeliJournalof EmergencyMedicineVol 3, No.
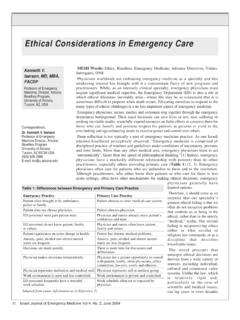
6 3, September2003. Phenytoin for Diphenhydramine Toxicity m a s s e sw e r e f e l t . T h e p u p i l s w e r e 4 m m a n d were normal. Her eyes were lr ll , closedand she was flexing all four limbs to pain. There were no gag or cornealreflexesand no doll's r l , Ir rl il , .-'l eye skin lesionswereobserved. A 12 lead electrocardiogram (figure l) showeda wide complex tachycardiawhich was interpretedat the time, and later confirmedby two cardiologists. as likely beinga ventriculartachycardia(VT). l l r W i thi n l 5 mi nutesof arri val to the E D NaHCO T. one ampule (50 ml. 88 meq) and two ampulesin , i11r1,,,i ,i;,,.-.;{. I L D5W @ 250 cc/h was also receivedactivatedcharcoal,50 g by nasogastric Fipure l. This is a l2 lead ECG of the putient discussetlirt this renort Drittr to tube.}
7 Triutment with nhent'toin. It 'tlte ol' rt'ide cotrrDle.\'tu<'lt't'<'urtliu (arrou's). The alsterisksindicote likelv This ECG vits inlerni'eted ' bt' A r t e r i a l b l o o d g a s e s( A B G ) f i v e m i n u t e sa f t e r tvvoc' representiig' ' Ventriculur Tu<'hyt'urtliu. admi ni strati onof N aH C OTw er pH 'pCO 2. 28 mmHg; mmHg; and -HCOr23meq/L. A. ,i t i 11' chest x-ray was normal. A half hour after arrival to the ED. initial blood work-up showed sodium (Na) 139 meq/L;. Potassium(K) meq/L; Chloride (CI. 100meq/L and meq/L. A l cohol , acetyl sal i cyl i caci d and acetam inophen levels were not tricyclic antidepressant screeningwas toxicology screening was not done. Thirty five minutesafter arriving in the ED, runs of VT the next 45 minutes,despite l i d o c a i n e ,a 3 m g / K g I V b o l u s.)
8 F o l l o w e d b y Ficure 2. This a I2 teud ECG of the same Dutienl 4 mg/min infusion and anotherampuleof NaHCOT. inlusion lluu l,lluston hutl sIoJrD(u. stoppetl. There ure n(, I nere ure long,er nins ol v nlitIOnRer tliar the QT inteiial is .still ahnonnullt long. bei ng admi ni stered,runs of V T conti nu I. 40 meq [V was administeredand a repeatABG. showedpH ; pCO:26mmHg; O:188 mmHg; -HCO,22meqil- and K meqlL. In order to treat the VT, phenytoin750mg IV was administeredover 30 minutes,the infusion beginningtwo hours after arrival in the ED. No further VT was observedonce the infusion had stopped. Procainamide,amiodaroneand bretylium were not consideredfor treatmentbecause the ECG had a prolongedQT interval suggestiveof type Ia antiarrhythmictoxicity and thesedrugsare contraindicatedin this circumstance.))]
9 A CT scanof the headwas normal. One hour after the phenytoininfusion beganthe BP was notedto be only 87/51 mmHg. Following IV NS 500 ml bolus,the BP was 92178mmHg with a sinustachycardiaof 100 beats/min.(Figure2). A repeatdoseof activatedcharcoal50 g was given and the patientwas transferredto the intensivecare unit. She was extubatedlater that day. She admitted to taking more than twenty 50mg capletsof Sominex,,.Eventuallyshe was transferredto psychiatrywith no known long term neurologicor cardiacsequelae. Discussion Diphenhydramine is an Hl 's toxic actionswith exceptionto its Cardiac effects,are primarily due to its anticholinergicproperties(3). Toxicity is common (4). Anticholinergicpoisoningusuallypredomina tes (4).
10 Tachyarrhythmias,bradyarrhythmias, fibrillation, bundle branchblocks, hypotensionand completecardiovascularcollapsehave been 2003'ltnugo ,3 ll)rl ,3 i'l9lnTilNlgt) r)Nlurn nDil tn) 5. Phenytoin for Diphenhydramine Toxicity observedfollowing large diphenhydramineingestion(5). In most reportedfatal or life threatening cardiactoxicity presentsfollowing seizureactivity(3,4,6). In 1992 Clark and Vance (2) reporteda diphenhydramineintentionaloverdoseresult ing in progressiveloss of consciousness, then ventriculartachycardia with a normal blood that the TCA overdosewas the cause of the clinical presentation, they alkalinized(pH> )the patientwith an IV NaHCO, bolus and infusion and observed an abolition of the VT. No TCA ingestionwas found o n s e ru m a nal ysi sor hi story.