Transcription of Understanding asthma pathophysiology, diagnosis, and ...
1 Understanding asthma pathophysiology, diagnosis, and management Learn about new research findings and current treatment strategies for this common disorder. By Shari J. Lynn, MSN, RN, and Kathryn Kushto-Reese, MS, RN. A CHRONIC inflammatory airway from various host factors, environ- even though obvious signs and disorder, asthma is marked by air- mental factors, or a combination. symptoms of asthma may not al- way hyperresponsiveness with re- Host factors include gender, obesi- ways occur. current episodes of wheezing, ty, and genetics. Genetic factors in- Bronchospasms, edema, exces- coughing, tightness of the chest, clude atopy. Defined as a genetic sive mucus, and epithelial and and shortness of breath. Typically, tendency to develop allergic dis- muscle damage can lead to bron- these episodes are associated with eases, such as asthma and allergic choconstriction with broncho- airflow obstruction that may be re- rhinitis, atopy commonly is linked spasm.
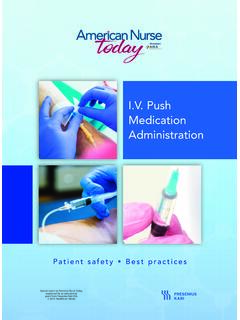
2 Defined as sharp contrac- versed spontaneously or with to an immunoglobulin E (IgE) me- tions of bronchial smooth muscle, treatment. diated response to allergens. bronchospasm causes the airways asthma affects approximately to narrow; edema from microvascu- 300 million people around the Pathophysiology lar leakage contributes to airway world. In children, males have a Understanding asthma pathophysi- narrowing. Airway capillaries may higher asthma risk; in adults, fe- ology helps you understand how dilate and leak, increasing secre- males have a higher prevalence. the condition is diagnosed and tions, which in turn causes edema Experts believe asthma results treated. Our knowledge of asthma and impairs mucus clearance. (See pathogenesis has changed dramati- How bronchospasm constricts the cally in the last 25 years, as re- airway.)
3 Searchers have found various asth- asthma also may lead to an in- ma phenotypes. crease in mucus-secreting cells asthma involves many patho- with expansion of mucus-secreting physiologic factors, including glands. Increased mucus secretion bronchiolar inflammation with can cause thick mucus plugs that airway constriction and resist- block the airway. Injury to the ep- ance that manifests as epi- ithelium may cause epithelial peel- sodes of coughing, shortness ing, which may result of breath, and wheezing. in extreme airway asthma can affect the tra- impairment. chea, bronchi, and bronchi- Loss of oles. Inflammation can exist the July 2015 American Nurse Today 49. How bronchospasm constricts the airway These illustrations compare a normal airway (left) to an asthmatic one (middle) and an asthmatic airway during an asthma attack (right).
4 Volve an IgE response. It may have fewer obvious triggers and usually occurs in adults, possibly secondary to a viral infection. Diagnosis asthma diagnosis goes beyond symptoms, such as coughing, chest tightness, wheezing, and dysp- nea and even beyond signs and symptoms that worsen at night and improve after treatment. Diagnosis may require pulmonary function tests (PFTs) and peak expiratory flow (PEF) measurements. With asthma , the ratio of forced expira- tory volume in 1 second (FEV1) to forced vital capacity (FVC, also called FEV1%) typically declines. asthma symptoms can be re- versed by a rapid-acting beta2- agonist, such as albuterol, as meas- ured by spirometry. The general- epithelium's barrier function allows ly acceptable response to beta2- allergens to penetrate, causing the agonists is a 12% or 200-mL increase airways to become hyperrespon- sive a major feature of asthma .
5 Without proper treatment in FEV1 or FVC. PEF measurements not only aid diagnosis but also help The degree of hyperresponsiveness depends largely on the extent of and control, asthma may clinicians monitor the disease. Some patients with asthma signs inflammation and the individual's and symptoms may have normal immunologic response. cause airway remodeling. PFT results. They may need fur- asthma also causes loss of en- ther diagnostic testing, such as air- zymes that normally break down way response testing using a bron- inflammatory mediators, with ensu- pollen, pet dander, smoke, or chial challenge. (See Bronchial ing reflexive neural effects from certain drugs or foods. On ex- challenge.). sensory nerve exposure. Without posure to a trigger, excessive re- Clinicians must rule out other proper treatment and control, asth- lease of IgE occurs, which initi- conditions that may decrease FEV1.
6 Ma may cause airway remodeling ates B-lymphocyte activation. and cause signs and symptoms that leading to changes to cells and tis- IgE binds to cells related to in- mimic asthma . These conditions in- sues in the lower respiratory tract; flammation. This action causes clude vocal cord dysfunction, gas- these changes cause permanent fi- release of inflammatory media- troesophageal reflux disease, is- brotic damage. Such remodeling tors (such as chemokines, nitric chemic cardiac pain, chronic may be irreversible, resulting in oxide, prostaglandin D2, cyto- obstructive pulmonary disease, progressive loss of lung function kines, histamine, and leuko- heart failure, upper-airway obstruc- and decreased response to therapy. trienes), in turn triggering tion, cystic fibrosis, hyperventila- airway inflammation and bron- tion, and foreign-body aspiration.
7 Classifying asthma choconstriction. Women who Viral respiratory infections may asthma may be atopic, nonatopic, smoke during pregnancy may lead to asthma exacerbations or or a combination. predispose their unborn chil- contribute to eventual develop- Atopic asthma begins in child- dren to higher IgE levels, caus- ment of the disorder. hood and is linked to triggers ing hyperresponsiveness and that initiate wheezing. It may asthma development. Exposure Management arise after exposure and re- to pollution may have the same asthma management involves both sponse to a specific allergen, effect. acute and long-term treatment. such as dust mites, grass or tree Nonatopic asthma doesn't in- Medication selection hinges on the 50 American Nurse Today Volume 10, Number 7 patient's age, disease severity, and comorbidities. Bronchial challenge Be sure to obtain a complete In the bronchial challenge, a patient with airway hypersensitivity inhales an aggra- medication history before the pa- vating agent with the potential to cause bronchoconstriction.
8 The inhaled agent tient starts taking asthma medica- may act directly (such as inhaled histamine or methacholine) or indirectly (such as tions. Some drugs, including beta- mannitol). The agent's histamine properties increase mucus production and bronchocon- blockers, angiotensin-converting striction. Cholinergic properties of methacholine cause wheezing and shortness of enzyme inhibitors, cholinergics, breath. The mannitol inhalation challenge (approved in some countries) may and nonpotassium-sparing diuret- cause airway narrowing in asthmatic patients by altering the osmolarity of airway ics, may be contraindicated for surface liquid, in turn resulting in mast cell granulation and release of inflammato- patients receiving certain asthma ry mediators. agents. In these tests, a decrease of 15% to 20% from the patient's baseline forced ex- piratory volume in 1 second indicates asthma .
9 Rescue (quick-relief) drugs Meant for short-term symptom re- lief, rescue drugs cause bronchodi- tion. Urge patients to receive an- lation and are used mainly to pre- nual vaccinations, as asthma in- vent or treat an asthma attack. They begin working within min- Be sure to obtain a creases the risk of complications from respiratory diseases, such as utes and may remain effective for pneumonia and influenza.. up to 6 hours. Potential side ef- complete medication fects include jitteriness and palpita- Selected references tions. Rescue drugs include iprat- ropium bromide inhaler (Atrovent), history before the patient asthma overview. American Academy of Aller- gy asthma and Immunology. conditions-and- short-acting beta2-agonists, and oral corticosteroids. starts taking asthma Corbridge S, Corbridge TC. asthma in ado- lescents and adults.
10 Am J Nurs. 2010;. Ipratropium bromide, an anti- 110(5):28-38. cholinergic, may be given in medications. Fanta CH. Treatment of acute exacerbation combination with short-acting of asthma in adults. Last updated February 5, beta2-agonists in some cases. 2015. Beta2-agonists used for quick re- teroid and an LABA. These drugs -of-acute-exacerbations-of- asthma -in-adu lts lief include albuterol, leval- may take days or weeks to reach Global Initiative for asthma . Pocket Guide buterol, metaproterenol, and maximal effect. for asthma Management and Prevention (for terbutaline. Leukotriene modifiers help pre- Adults and Children Older than 5 Years). Updated 2015. Oral corticosteroids, such as vent symptoms for up to 24 hours. uploads/ prednisone and methylpred- LABAs, which may last up to 12. Johnson J. asthma assessment tips. J Nurse nisolone, sometimes are used hours, usually are given in combi- Pract.