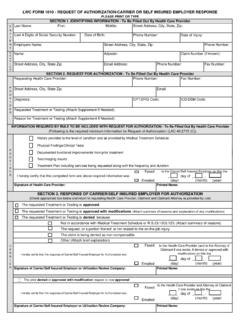
PLEASE PRINT OR TYPE SECTION 1. IDENTIFYING …
Faxed Emailed Faxed Emailed Faxed Emailed C A R R I E R P R O V Appeal of Suspension to Medical Services Section by Health Care Provider I hereby certify that this First Request and accompanying Form 1010A was _____ day of _____ , _____ (day) (month) (year)
Download PLEASE PRINT OR TYPE SECTION 1. IDENTIFYING …

Information
Domain:
Source:
Link to this page:
Documents from same domain
Unemployment Insurance Tax Guide for Employers
www.laworks.netUnemployment Insurance Tax Guide for Employers i Vision We will make Louisiana the best place in the country to get a job or grow a business, and our goal is to be

LaWATS- Manual Update - 07062017
www.laworks.netINSTRUCTIONS FOR EMPLOYERS Create UI Online Services Account Login Before You Begin 1. You must have an unemployment …
SNAP Requirement to Register for Work with …
www.laworks.netSNAP Requirement to Register for Work with Louisiana Workforce Commission (LWC) February 2014 . Presented by Allison Shortess . SNAP Director

CHAPTER 4: LRS TECHNICAL ASSISTANCE & …
www.laworks.netChapter 4, Part 412.14 Page 2 of 21 B. The Regional Manager is responsible for assigning a Counselor or Supervisor to serve as a Supervising Counselor for each of the region’s supported employment CRP

Rights & Responsibilities for Employees & …
www.laworks.netRights & Responsibilities for Employees & Employers: | 1 Page RIGHTS AND RESPONSIBILITIES FOR EMPLOYEES AND EMPLOYERS - This Office of Workers’ Compensation Administration’s Rights and Responsibilities brochure is sent
Career Planning Guide - Louisiana Workforce …
www.laworks.netLOUISIANA CAREER PLANNING GUIDE 1 Dear Students, Parents, and Educators: We are pleased to present the L i ia a Ca ee Pla i g G …
NOTE: This form is not an Employment Certificate.
www.laworks.netNOTE: This form is not an Employment Certificate. The process for employing a minor, under the age of 18, involves a two-part process: 1. After the employer completes this application, the minor must have a parent sign the Parent’s
CHAPTER 4: LRS TECHNICAL ASSISTANCE & …
www.laworks.netChapter 4, Part 414 Page 1 of 5 . Federal regulations require that the State Agency assume responsibility for placement of all job-ready consumers receiving vocational rehabilitation services.
Disputed Claim for Medical Treatment - LAWorks
www.laworks.net1 E-Mail to: mgd1009@lwc.la.gov 1. Last four digit of Social Security No. Fax to: OWCA – Medical Services 2. Date of Injury/Illness - -
LOUISIANA WORKERS’ COMPENSATION SECOND …
www.laworks.netpage _____ of_____ sib form d (10/17) louisiana workers’ compensation second injury board post‐hire/conditional job offer knowledge questionnaire
Related documents

Aetna Medicare Advantage Plan non -contract provider ...
www.aetna.comAetna Medicare Advantage Plan non -contract provider payment appeal process You have the right to appeal our payment denial by initiating the Medicare Managed

Practitioner and Provider Compliant and Appeal Request
www.aetna.comPractitioner and Provider Complaint and Appeal Request NOTE: Completion of this form is mandatory. To obtain a review submit this form as well as information that will support your appeal…

COLORADO ACCESS CLAIM APPEAL FORM
www.coaccess.comcoaess.o 1-800-511-5010 C COLORADO ACCESS CLAIM APPEAL FORM All fields are required. If information is missing, the appeal will not be processed and will be returned to the address

State of California Division of Workers’ Compensation ...
www.dir.ca.govDWC Form SBR-1 (Effective 2/2014) Page 1 State of California Division of Workers’ Compensation Provider’s Request for Second Bill Review

Request for Claim Review Form
www.hcasma.orgMassachusetts Administrative Simplification Collaborative–Request for Claim Review V1.01 Request for Claim Review Form Today’s Date (MM/DD/YY): Health Plan Name:

Request for Claim Review Form
www.hcasma.orgThis guide will help you to correctly submit the Request for Claim Review Form. The information provided is not meant to contradict or replace a payer’s

PROVIDER APPEAL REQUEST FORM - lmchealthplans.com
www.lmchealthplans.com07/2016 PROVIDER APPEAL REQUEST FORM This form should be used if you disagree with the outcome of your claims inquiry or have additional information which

Texas Standard Prior Authorization Request Form for …
www.bcbstx.comTitle: Texas Standard Prior Authorization Request Form for Health Care Services Author: Texas Department of Insurance Keywords: prior authorization request form, NOFR001, SB 1216
Related search queries
Aetna, Provider, Appeal, Practitioner and Provider Compliant and Appeal Request, Appeal Request, COLORADO ACCESS CLAIM APPEAL FORM, California Division of Workers’ Compensation, California Division of Workers’ Compensation Provider, Request for Second Bill Review, Request for Claim Review Form, Request, Review Form, PROVIDER APPEAL REQUEST FORM, Texas Standard Prior Authorization Request Form