Authorization For Medication Administration
Found 9 free book(s)
Child Care Medication Authorization Form
wvearlychildhood.orgchild care center) personnel to administer the medication named above to my child in the manner as stated. I release any liability in relation to the administration of this medication. I also acknowledge that I, the parent/guardian , have given the first dose of this medication …

Specialty Medication Precertification Request
www.aetna.comSpecialty Medication Precertification Request Aetna Precertification Notification Phone: 1-866-752-7021 ... D. DISPENSING PROVIDER/ADMINISTRATION INFORMATION Place of Administration: Self-administered . Physician’s Office . ... Any person who knowingly files a request for authorization of coverage of a medical procedure or service with the ...

Authorization for the Administration of Medication by ...
portal.ct.govParents/guardians requesting medication administration to their child shall provide the program with appropriate written authorization(s) and the medication before any medications are administered. Medications must be in the original container and …

SCHOOL MEDICATION PRESCRIBER/PARENT …
www.childrensal.orgPrescription Medication must be registered with School Nurse or trained Medication Assistants. Prescription medication must be properly labeled with student’s name, prescriber’s name, name of medication, dosage, time intervals, route of administration and the date of drug’s expiration when appropriate.

OCA Official Form No.: 960 AUTHORIZATION FOR RELEASE …
www.nycourts.govof the HIPAA-compliant Authorization Form to Release Health Information Needed for Litigation This form is the product of a collaborative process between the New York State Office of Court Administration, representatives of the medical provider community in New York, and the bench and bar, designed to produce a standard official form that
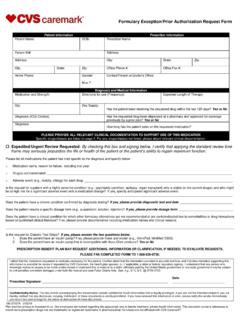
Formulary Exception/Prior Authorization Request Form
www.caremark.comMedication and Strength: Directions for use (Frequency): Expected Length of Therapy: Qty: Day Supply: PLEASE PROVIDE ALL RELEVANT CLINICAL DOCUMENTATION TO SUPPORT USE OF THIS MEDICATION Solely providing demographic and drug information may not constitute a sufficient request for coverage. Specific drugs/classes are listed on page 2.

FACT SHEET FOR HEALTHCARE PROVIDERS EMERGENCY USE ...
pi.lilly.comThe U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) to permit the emergency use of baricitinib for treatment of coronavirus disease 2019 (COVID-19) in hospitalized adults and pediatric patients 2

Informed Consent Required for Psychotherapeutic ...
www.caremark.comAs of September 1, 2011, Florida Medicaid, a divisionof the Agency for Health Care Administration(AHCA) , requires informed consent from the parent or legal guardian of children age 12 and under who are prescribed psychotherapeutic medications. CVS/caremark will provide the following or a similar message to help remind

PRESCRIPTION D PRIOR AUTHORIZATION REQUEST FORM
www.empirepharmacy.comPage2of2 New 08/13 Form 61‐211 PRESCRIPTION DRUG PRIOR AUTHORIZATION REQUEST FORM Patient Name: ID#: Instructions: Please fill out all applicable sections on both pages completely and legibly.Attach any additional documentation that is important for the review, e.g. chart notes or lab data, to support the prior authorization request.
Similar queries
Child Care Medication Authorization Form, MEDICATION, Administration, Specialty Medication Precertification Request, Specialty Medication Precertification Request Aetna, Authorization, Authorization for the Administration of Medication, Medication administration, SCHOOL MEDICATION PRESCRIBER/PARENT, HIPAA, Baricitinib, PRIOR AUTHORIZATION REQUEST FORM