Direct referral form
Found 6 free book(s)
PATIENT SELF-REFERRAL PHYSIOTHERAPY REQUEST FORM …
www.wellside.org.ukPHYSIOTHERAPY REQUEST FORM PHYSIO DIRECT 01480 434980 Current hours of operation are Mon –Fri 8.15am-12.15pm. TELEPHONING THIS NUMBER IS THE QUICKEST WAY TO ACCESS OUR

DIRECT REFERRAL FORM - Preferred IPA of California
www.preferredipa.com–Yearly D iabetic Exams or Glaucoma screening- (Vision Care is Health Plan Responsibility for most plans)
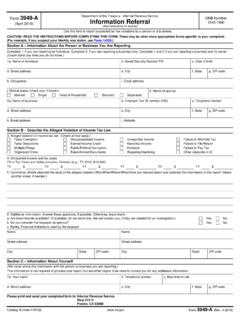
Form 3949-A Information Referral - Internal Revenue Service
www.irs.govCatalog Number 47872E. www.irs.gov Form 3949-A (Rev. 4-2016). Form 3949-A (April 2016) Department of the Treasury - Internal Revenue Service Information Referral (See instructions on reverse)

IV-D Child Support Services Application/Referral
www.michigan.govDHS-1201 (Rev. 6-15) Previous edition may be used. MS Word 1 IV-D CHILD SUPPORT SERVICES APPLICATION/REFERRAL FOR OFFICE USE ONLY Michigan Department …

OPTICAL BENEFIT FORM - C.F. Sharp Group
www.cfsharp.comTO: Executive Optical Inc. “Love your Eyes” Branch: _____ For additional inquiries: EO Corporate Accounts Department Help desk: corpaccount2@eo-executiveoptical.com

INSTRUCTIONS - services.gileadhiv.com
services.gileadhiv.comBy signing this form, I certify that I am prescribing Gilead medication for the patient identified in Section 3. I certify that this prescription medication is medically necessary for the