For Reconsideration
Found 6 free book(s)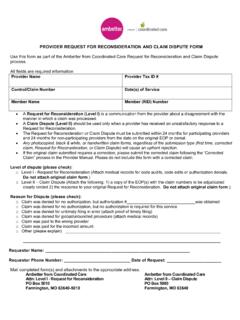
Provider Request for Reconsideration and Claim Dispute Form
ambetter.coordinatedcarehealth.com• A Request for Reconsideration (Level I) is a communication from the provider about a disagreement with the manner in which a claim was processed. • A Claim Dispute (Level II) should be used only when a provider has received an unsatisfactory response to a Request for Reconsideration.

Single Paper Claim Reconsideration Request Form
www.uhcprovider.com2 A claim reconsideration request is not a claim appeal and does not alter or toll the deadline for submitting an appeal on any given claim. Claim reconsideration requests cannot be submitted for member plans sitused in Maryland. PCA-1-20-04206-PO-WEB_01142021 • • ...

UHCCP Claims Reconsideration Form - UHCprovider.com
www.uhcprovider.comClaims Reconsideration Request Form To request reconsideration of a claim, please complete and mail this form along with a copy of the related provider remittance advice or explanation of benefits to the following address. Please submit a separate form for …

Lender Reconsideration of Value Request SOP
benefits.va.govReconsideration of Value Request Requirements The value estimate on a NOV may be changed if the change is clearly warranted and fully supported by real estate market or other valid information which would be considered adequate and reasonable by …

MEDICARE RECONSIDERATION REQUEST FORM — 2nd …
www.cms.govMEDICARE RECONSIDERATION REQUEST FORM — 2nd LEVEL OF APPEAL. Beneficiary’s name (First, Middle, Last) Medicare number . Date the service or item was received (mm/dd/yyyy) Item or service you wish to appeal . Date of the redetermination notice (mm/dd/yyyy) (please include a copy of the . notice with this request)

What Should You Know About - IRS tax forms
www.irs.govAn Audit Reconsideration is a process used by the Internal Revenue Service to help you when you disagree with the results of an IRS audit of your tax return, or a return created for you by the IRS because you did not file a tax return as authorized by the Internal Revenue Code 6020(b).