Search results with tag "Medical condition"

CSEP-CPT Health Screening Tool for Clients with One ...
www.csep.caCSEP-CPT Health Screening Tool for Clients with Medical Conditions (Sept 20, 2017) v2 Page 1 of 2 CSEP-CPT Health Screening Tool for Clients with One Medical Condition A CSEP-CPT can work with clients who have one diagnosed medical condition that is “stable” or determined to be at a lower risk for an adverse event during exercise.
Certification of Health Care Provider for Family Member’s ...
www.yccd.edu2.Is the medical condition pregnancy? ___ No ___Yes. If so, expected delivery date: _____ 3.Describe other relevant medical facts, if any, related to the condition for which the patient needs care (such medical facts may include symptoms, diagnosis, or any regimen of continuing treatment such as the use of specialized equipment):
CUSTOMER MEDICAL REPORT - Virginia
www.dmv.virginia.govA patient self-reported on their application a medical condition or a medication that may indicate a medical condition that DMV evaluates for driver safety. 3. Based on the examination that you conduct, please complete the parts of the MED 2 that pertain to …

DURABLE MEDICAL EQUIPMENT, PROSTHETIC, ORTHOTIC, …
www.emedny.orgDurable Medical Equipment . Durable medical equipment (DME) is defined as devices and equipment, other than prosthetic or orthotic appliances, which have been ordered by a practitioner in the treatment of a specific medical condition and which have all the following characteristics: can withstand repeated use for a protracted period of time;

ICHIGAN DEPARTMENT OF CORRECTIONS FAMILY MEDICAL …
www.michigan.gov8. Is the medical condition pregnancy? Yes No If yes, expected delivery date: 9. Based on the essential job functions in the attached job description (or based upon the employee’s own description of his or her job functions if no job description is provided), is the employee unable to perform any of the job functions due to the condition?
SECTION I - EMPLOYER - DOL
www.dol.govFor the medical condition(s) checked in Part A , complete all that apply . Several questions seek a response as to the frequency or duration of a condition, treatment, etc. Your answer should be your . best estimate . based upon your medical knowledge, experience, and …

TSA Notiication Card: Individuals with Disabilities …
www.tsa.govTSA Notiication Card: Individuals with Disabilities and Medical Conditions I have the following health condition, disability or medical device that may affect my screening:

Florida Workers' Compensation Uniform Medical Treatment ...
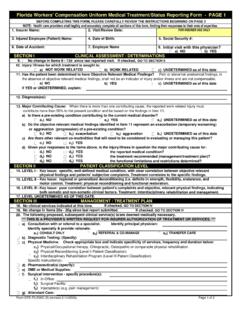
myfloridacfo.comthe reported medical condition? the functional limitations and restrictions determined? Are there other relevant co-morbidities that will need to be considered in evaluating or managing this patient? Given your responses to the Items above, is the injury/illness in question the major contributing cause for: d 3) NO If checked, GO TO SECTION IV
Florida Workers' Compensation Uniform Medical Treatment ...
www.myfloridacfo.comthe reported medical condition? the functional limitations and restrictions determined? Are there other relevant co-morbidities that will need to be considered in evaluating or managing this patient? Given your responses to the Items above, is the injury/illness in question the major contributing cause for: d 3) NO If checked, GO TO SECTION IV

Provider Manual Blue Cross Community MMAI (Medicare- …
www.bcbsil.coman independent licensee of the Blue Cross and Blue Shield Association. ... a Presidential (major) disaster declaration, a declaration of emergency or disaster by a governor or an announcement of a public health emergency by the Secretary of ... they have an emergency medical condition should be directed to seek emergency services immediately.

Exercise Pre-Screening Questionnaire
www.physicalactivityaustralia.org.auI believe to the best of my knowledge that all of the information I have provided on this tool is accurate. In the case that my medical condition changes over the course of my training I will inform my trainer and fill out a new exercise pre-screening questionnaire. Client signature: Trainer signature: Date: Date:

CDHO Factsheet COPD - College of Dental …
www.cdho.org69 Bloor St. E, Suite 300, Toronto, ON M4W 1A9 t: 416-961-6234 tf: 1-800-268-2346 f: 416-961-6028 www.cdho.org Disease/Medical Condition CHRONIC OBSTRUCTIVE
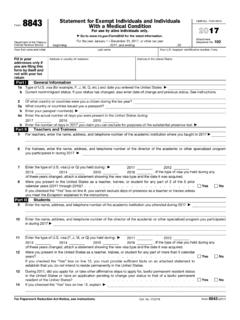
2017 Form 8843
www.irs.govForm 8843 Department of the Treasury Internal Revenue Service Statement for Exempt Individuals and Individuals With a Medical Condition For use by …

Medical Condition Notification Form - Transport for NSW
www.nsw.gov.auMedical Condition Notification Form Catalogue No. 45071651 Form No. 1628 (03/2017) Assessment of fitness to drive Patient details (please print) I have examined the above named patient in accordance with the relevant national medical standards as set

MEDICAL EXCUSE FROM JURY DUTY BASED ON SERIOUS …
www.iowacourts.govPLEASE DO NOT PROVIDE MEDICAL RECORDS OR MEDICAL INFORMATION. PLEASE COMPLETE THE CERTIFICATION BELOW I hereby swear and affirm that the individual identified above is my patient, and that he/she has a serious medical condition at the present time that prevents him/her from being able to appear for jury duty.
Similar queries
Health Screening Tool for Clients with One, Health Screening Tool for Clients with Medical, Health Screening Tool for Clients with One Medical Condition, Clients, Medical condition, MEDICAL, Condition, Equipment, CUSTOMER MEDICAL REPORT, Virginia, Medical equipment, Medical Conditions, Managing, Provider Manual Blue Cross Community MMAI Medicare, Licensee, Declaration, Screening questionnaire, Tool, CDHO Factsheet COPD, Form 8843, Internal Revenue Service, MEDICAL EXCUSE FROM JURY DUTY