Search results with tag "Form fax"
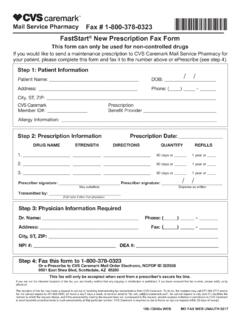
FastStart New Prescription Fax Form - Caremark
www.caremark.comFastStart® New Prescription Fax Form This form can only be used for non-controlled drugs If you would like to send a maintenance prescription to CVS Caremark Mail Service Pharmacy for your patient, please complete this form and fax it to the number above or ePrescribe (see step 4). Fax # 1-800-378-0323 Step 3: Physician Information Required

PRESCRIPTION DRUG MEDICATION REQUEST FORM FAX ... - …
www.highmarkblueshield.com1. Submit a separate form for each medication. 2. Complete ALL information on the form. NOTE: The prescribing physician (PCP or Specialist) should, in most cases, complete the form. 3. Please provide the physician address as it is required for physician notification.

Georgia - Outpatient Medicaid Prior Authorization Fax Form
www.pshpgeorgia.comPRIOR AUTHORIZATION FAX FORM Complete and Fax to: 1-866-532-8834. Request for additional units. Existing Authorization . Units. Standard Request . Urgent Request - I certify this request is urgent and medically necessary to treat an injury, illness or condition (not life threatening) within 48 hours
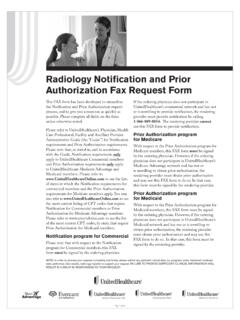
Radiology Notification and Prior Authorization Fax Request ...
www.corridorradiology.comFAX form to do so. In that case, this form must be signed by the rendering provider. NOTE: In order to process your request completely and timely, please submit any pertinent clinical data (i.e. progress notes, treatment rendered, tests performed, labs results, radiology reports) to support your request. FAILURE TO PROVIDE SUFFICIENT CLINICAL ...

SECONDARY AUTHORIZATION REQUEST (SAR) FORM Fax …
www.triwest.comsecondary authorization request (sar) form fax to 1-866 -259 0311. section i: patient information last name: first name:
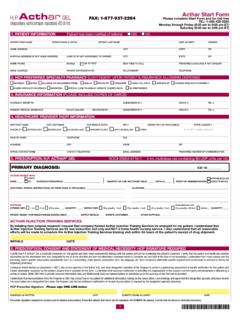
Acthar Start Form FAX: 1-877-937-2284 Please …
www.acthar.com2 7. DIAGNOSIS AND MEDICAL INFORMATION OTHER RELEVANT CLINICAL INFORMATION Diagnosis Please select diagnosis and responses to associated …