Search results with tag "Enrollment form"

,.1/Z HEALTH AND ENROLLMENT FORM - District Council 37
www.dc37.netdependent information, please submit a "Change of Status Form". • Sign and date the Enrollment Form. • Please send the Enrollment Form to the following address: DC 37 Health and Security Plan 125 Barclay Street, Room 811 New York, NY 10007 Attn: Eligibility Enrolbnent Unit Fax# 212 815-1649 If you have any questions, feel free to contact ...

Kaiser Permanente Medicare Advantage/Senior Advantage …
healthplans.kaiserpermanente.orgGroup Medicare Election/Enrollment Form . Filling out and returning the enrollment form is your first step to becoming a Kaiser Permanente Medicare Advantage/Senior Advantage member. If you and your spouse are both applying, you’ll each need to fill out a separate form. For help completing the enrollment form, call

New York State Medicaid Enrollment Form - …
www.emedny.orgclaims submitted for services, care, or supplies furnished before the enrollment date authorized by the Department of Health. If you have any questions, contact the eMedNY Call Center at (800) 343-9000. Consider printing the Instructions to Complete Enrollment Form before continuing. Please complete pages 2 through 8; form must be completed in its

2022 Enrollment Form
healthy.kaiserpermanente.org2022 Enrollment Form Northern California or Southern California Region Individual Plan ... • If you want to join a plan during fall open enrollment (October 15–December 7), the plan ... with Medicare, who may use it to track my enrollment, to make payments, and for other purposes allowed by Federal law that ...

EPS EFT Enrollment Authorization Agreement - Optum
www.optum.comThe enrollment form MUST be signed by authorized healthcare individuals. Practitioner (MD, DO, DC, DDS, PhD, etc) Corporate Officer or Authorized Manager (CEO, CFO, Office Manager, etc) Written signature of person submitting enrollment: Printed name of person submitting enrollment: Print title of person submitting enrollment:

The Merck Access Program Enrollment Form
www.merckaccessprogram.com1/17 The Merck Access Program Enrollment Form Phone: 855-257-3932, Fax: 855-755-0518 The Merck Access Program PO Box 29067 Phoenix, AZ 85038 To geT sTarTed, compleTe The enrollmenT form and fax iT To 855-755-0518.

Questions? Return completed form to Enrollment …
modelaircraft.orgEnrollment Form for Membership Questions? For help completing this form, contact AMA at (800) 435-9262. www.modelaircraft.org Return completed form to

AstraZeneca Access 360™ Enrollment Form
www.myaccess360.comAstraZeneca Access 360™ Enrollment Form 4 Prescriber Authorization I authorize Access 360 program to convey the attached prescription on my behalf to the pharmacy chosen above and to receive information on the status and related matters. By signing on Page 3, I certify that the medicine prescribed on this form is medically necessary
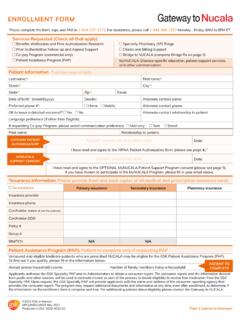
Gateway to NUCALA Enrollment
nucalahcp.comPlease complete the form, sign, and FA to 1-844-23-312. For assistance, please call 1-844-468-2252 Monday - Friday, 8AM to 8PM ET. ... please submit an actual prescription along with this enrollment form. ... • Prescriber signature below is required for Rx and/or enrollment • Specialty Pharmacy selection is subject to health plan requirements
Section 125 Cafeteria Plan Summary Plan Document (SPD)
www.employersresource.comYou should complete an Enrollment Form during the Open Enrollment Period prior to each Plan Year. If you fail to return your Enrollment Form, you will be deemed to have made the elections specified in Appendix A below. 9. Can I change my election during the Plan Year? Generally, you cannot change your elections during the Plan Year. However ...

Taltz Enrollment Form - Taltz® (ixekizumab)
www.taltz.comTaltz® (ixekizumab) Dermatology Savings and Support Enrollment Form Please complete and fax this form to 1-844-344-8108 If you have any questions, please call Taltz Together™ at 1-844-TALTZ-NOW (1-844-825-8966), Monday-Friday 8am – 10pm ET

ARISTADA Patient Enrollment Form
www.aristadacaresupport.comenrollment form is complete and accurate to the best of my knowledge. I understand that ... Preferred Pharmacy name Phone # Fax # If Benefit Verification results specify a pharmacy other than preferred pharmacy, ... 02451, 1-844-464-7171. Withdrawal of this authorization will end my consent to further disclosures of Information authorized ...

Synagis Respiratory Syncytial Virus (RSV) Enrollment Form
www.uhcprovider.comDoc#: PCA-1-011017-06072018_06202018 1 of 2 Synagis® Respiratory Syncytial Virus (RSV) Enrollment Form . Today’s date: / / Need by date: / / Please complete this entire form for UnitedHealthcare Community Plan members needing a Synagis prescription and fax it to

Leap Enrollment Form - Official Patient Site
www.letairis.com® Prescription and LEAP Patient Support Enrollment Form Please complete all fields on this form to prevent any delays in shipment of Letairis to your patient and fax to 1-888-882-4035. ... Prescribers and all female patients must be enrolled in the REMS program prior to initiating treatment. LETAIRIS: 5 mg tablets (30 tablets) PO QD Refills ...

Prescriber Only Enrollment Form - LaMedicaid.com
www.lamedicaid.comENROLLMENT PACKET FOR . THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Prescriber Only . Enrollment Form (All Inclusive Packet)

ELECTRONIC FUNDS TRANSFER (EFT) ENROLLMENT FORM …
sites.deltadentalok.orgPublic Revised 8/6/12 ELECTRONIC FUNDS TRANSFER (EFT) ENROLLMENT FORM Direct Deposit for Delta Dental of Oklahoma Please check one. New Authorization: (complete sections A, B, C, and F) Changes to existing authorization: (complete sections A, B, D and F) Cancellation: (complete sections A and E) Please return this form to the following address or fax number:

403(b) ENROLLMENT FORM - CalSTRS
www.calstrs.com403(b) enrollment form /page 3 of 6 plan # school district 400396 abc unified 400947 academia semillas del pueblo 401788 academy of the redwoods 400306 acalanes union high

Government Tax Payment & Filing Service Enrollment
www.scotiabank.comGovernment Tax Payment & Filing Service Enrollment Thank you for your interest in Scotiabank's Government Tax Payment and Filing Service (PFS). This enrollment form is for use by Corporate and

Universal Enrollment and Prescription Form
synagishcp.comNo Insurance Policyholder Full Name: ... please submit an actual prescription along with this enrollment form. 1 of 3. SIGN HERE. ... I may change my mind and cancel this Authorization at any time by calling 1-833-SYNAGIS (1-833-796-2447) or by notifying Sobi in writing at SYNAGIS CONNECT, PO Box 29076, Phoenix, AZ 85038-9076. ...

New York State Medicaid Enrollment Form
www.emedny.orgBy signing this enrollment form for participation in the New York State Medicaid Program, the Applicant/Provider understands and agrees to the following: As a Medicaid Provider you agree to comply with the rules, regulations and official directives of the Department

State Health Benefits Program Retiree Enrollment Form
www.dhrm.virginia.govInstructions for completing this form. Open Enrollment elections require completing Parts A, B, D and E. Address _____ City _____ State _____ Zip + 4 _____ 2 TYPE OF MEMBERSHIP Please select the membership type which describes the membership level for which you are enrolling: ...

ASIIS Enrollment Form
www.azdhs.gov• View Privilege means you can only look at the patient record and immunization record. • Edit Privilege means you can view, add and make changes to patient and immunization record. Name Email Address Privilege . ... ASIIS Enrollment Form Author: Ruth E. Penn Created Date:

Child Enrollment Form - HOME - Kidz Watch Sylvania OH
kidzwatch.netThis is a prescribed form which must be used by child care providers to meet the requirements to rules 5101:2- 12- 15, 5101:2- 13- 15, and 5101:2- 14- 04. This form must be on file at the program or home on or before the child’s first day of attendance and thereafter while the child is enrolled.

Patient Support Program & Patient Assistance Enrollment …
www.pfizeroncologytogether.comPatient Support Program Patient Assistance Enrollment Form Overview Pfizer Oncology Together is a personalized patient support program that offers resources for patients prescribed Pfizer Oncology medicines. We provide access and reimbursement support, as well as help identifying financial assistance options, so patients can get their

SAMPLE CHILDREN'S ENROLLMENT FORM Page 1of3
bessiechildcare.comSend your completed complaint form or letter to us by mail at U.S. Department of Agriculture, Director, Office of Adjudication, 1400 Independence Avenue, S.W., Washington, D.C. 20250-9410, by fax (202) 690-7442 or email at vcgram.intake@JJsda.gov.

State of Washington Medical Flexible Spending Arrangement ...
portal.naviabenefits.comPlease see the next page for important information about the above benefits. State of Washington Medical Flexible Spending Arrangement (FSA) & Dependent Care Assistance Program (DCAP) Enrollment Form

Electronic Data Interchange (EDI) Enrollment Form
www.cms.govModernization Act) covered under Health Insurance Portability and Accountability Act (HIPAA) Transactions and Code Sets or Section 1011 of the Medicare Modernization Act (MMA) legislation. A. The provider agrees: 1. That it will establish and maintain procedures and controls so that information concerning Medicare and/or Section

Patient Assistance Program Enrollment Form - PRALUENT
www.praluent.comPASS may ask for proof of income at any time for the purpose of audit/verification. If requested, I agree to provide proof of income within thirty (30) days of the request. Enrollment and continuation in the program is conditioned upon timely verification of income. In addition, I agree to notify PASS if my insurance situation changes.
EMPLOYEE BENEFITS POLICY AND PROCEDURES MANUAL
www.stancounty.comDELTA DENTAL CORE AND BUYUP PLANS VISION SERVICE PLAN VOYA RELIASTAR LIFE INSURANCE . 1. Employee’s legal spouse. *Unless the spouse is a Stanislaus County employee. ... ♦ Complete the County Benefit Enrollment Form selecting the options pertaining to the coverage level and plan choices along with dependent information. All dependent

RETIREMENT CHECKLIST
www.ndpers.nd.govMEDICARE PRESCRIPTION DRUG PLAN (PDP) INDIVIDUAL ENROLLMENT FORM (One required for each member that will be on the Dakota Retiree Plan and . cannot . ... RETIREE VISION\DENTAL INSURANCE ENROLLMENT, CHANGE, OR CANCEL (Complete if continuing, enrolling, or canceling coverage) 53504 ... (Rev. 11-2019) Page 2 .

See back of form for complete claimfiling instructions - UMR
member.umr.comExample - if your name was Eugene Smith on your enrollment form, claim must state Eugene, not Gene 5 Name,address and Tax ID number of the providerof service is required. If the provider's Tax ID number (9 digit number)is not on your copy of the receipt, you can contacttheir office to obtain it.

MERCK PATIENT ASSISTANCE PROGRAM ENROLLMENT …
merckhelps.comwith an acknowledgement of enrollment form receipt ... My Home My Physician’s Office Other Address ... including household income, is complete and accurate. I understand that program assistance will terminate if the program becomes aware of any fraud or if this medication is no longer prescribed for me. ...

“Patient Savings” Diagnosis-Based Assistance
www.needymeds.orgCelgene Patient Support ® Enrollment Form Phone 1-800-931-8691 Fax: 1-800-822-2496 Website www.celgenepatientsupport.com E-mail patientsupport@celgene.com Online enrollment availale at ww.celgenepatientsupport.com

CM-US-AQ-2119 AUVI-Q Direct Delivery Service Enrollment ...
www.auvi-q.comDirect Delivery Service Patient Enrollment Form Indication AUVI-Q® (epinephrine injection, USP) is a prescription medicine used to treat life-threatening allergic reactions, including anaphylaxis, in people who are at risk for or have a history of serious allergic reactions.
A Guide to Administering Your Com pany’s Health Insuran ce
download.paychex.comAn enrollment form is required in the following situations: New Hire & At Renewal– A n ew lyhi rd empl oee who ha s met the e ig b t requi ements and wi he to en Qualifying Event – An existing employee who experiences a qualifying event, has met the required

DIGITAL BANKING ENROLLMENT FORM - pnb.com.ph
www.pnb.com.phPHILIPPINE NATIONAL BANK DIGITAL BANKING SERVICE TERMS AND CONDITIONS The following Terms and Conditions shall govern the access and use of the Philippine National Bank Digital Banking Service (PNB Digital or the “Service”).

PATIENT AUTHORIZATION AND CONSENT - insupport.com
www.insupport.comP-BAG-US-00223 EXPIRY February 2020 Page 2 of 3 Fax INSUPPORT: 844-814-0669 Patient Certification for the INSUPPORT Copay Assistance Program (Private or Commercial insurance only) By signing this enrollment form, I certify that I have read, understand and agree to the Terms and Conditions of the INSUPPORT Copay Assistance

ENROLLMENT FORM - BENLYSTA
www.benlysta.comPrior Authorization Follow-up and Appeal Support Co-pay Program (commercial only) Patient Assistance Program (PAP) ... ©2021 GSK or licensor. BELBROC210011 May 2021 Produced in USA. 0002-0012-76. Please complete the form, ... Consult the patient’s payer for coding or documentation requirements. Diagnosis ICD-10 code*: Date of diagnosis (mm ...
Similar queries
Health, ENROLLMENT FORM, Change, Form, Plan, New York State Medicaid Enrollment Form, Enrollment, EMedNY, Open Enrollment, Optum, Practitioner, The Merck Access Program Enrollment Form, Program, Pharmacy, Ixekizumab) Dermatology Savings and Support Enrollment Form, Patient Enrollment Form, Phone, Patient, REMS program, Prescriber Only Enrollment Form, Prescriber Only . Enrollment Form, ELECTRONIC FUNDS TRANSFER (EFT) ENROLLMENT FORM, ELECTRONIC FUNDS TRANSFER (EFT) ENROLLMENT FORM Direct, Dental, 403(b) enrollment form, CalSTRS, School district, Unified, Government Tax Payment & Filing Service Enrollment, Scotiabank, Insurance, Provider, State Health Benefits Program, Electronic Data Interchange (EDI) Enrollment Form, Modernization Act, Medicare Modernization Act, Medicare, PASS, Audit, DELTA DENTAL, RETIREE, State, PROGRAM ENROLLMENT, Home, Direct, Employee, Service, Prior Authorization, Commercial, 2021, Requirements