Example: confidence
Search results with tag "Referral authorization request"
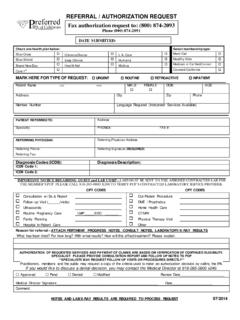
Phone (800) 874 -2091 DATE SUBMITTED:
www.preferredipa.comFax authorization request to: (800) 874-2093 Phone (800) 874 -2091 REFERRAL / AUTHORIZATION REQUEST . Check one health plan below: Select membership type: