Transcription of A colonic amoebic abscess mimicking colonic carcinoma
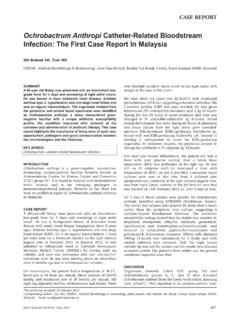
1 334 Med J Malaysia Vol 73 No 5 October 2018 SUMMARYA mebiasis is one of the major causes of diarrhea in thedeveloping countries and it can present with a wide range ofgastrointestinal symptoms depending on the phase ofinfection. We described a case of 50 year-old male patientwho presented with abdominal pain, diarrhea and right hemicolectomy for appendicular abscess withtumour over the ileum, histopathological examinationsrevealed numerous trophozoites of Entamoeba histolyticaina background of inflammations (Figure 1). Followingresection of the ameboma, he received intravenousmetronidazole treatment for total of two weeks amebiasis is an infection caused by a pathological intestinalprotozoan parasite, Entamoeba histolytica which occurs inabout 10% of the world s population.
2 It is commonly seen indeveloping or tropical countries. Intestinal amebiasis haswide clinical presentation ranging from asymptomatic todysentery and even extra-intestinal disease, such as brain orliver histolytica is transmitted via ingestion of theenvironmentally hardy cysts found in faecally contaminatedwater, fertilizer, soil or the contaminated hands of , faecal-oral transmission can alsooccur in the setting of anal sexual practices. The cysts canremain viable in the environment for weeks to ingestion of the cysts, they excyst in the colon,resulting in formation of trophozoites which can penetrateand invade the colonic mucosal barrier, leading to tissuedestruction, secretory bloody diarrhea and with amebic colitis often present with abdominalpain, bloody diarrhea and weight loss.
3 However, they canalso present with chronic diarrhea without weight loss, whichis usually neglected by elderly patients. Patients withadvanced age and those who are immunocompromised tendto suffer a more severe clinical course or present withcomplications like toxic E. histolytica colonic infection may cause theformation of mass-like granuloma (ameboma). Generally,ameboma present as a segmental, concentric mucosal lesionin the gastrointestinal tract causing lumen narrowing andthen leads to obstructive is a rarepresentation of invasive amebiasis and it is estimated tooccur in about of cases. It is often misdiagnosed to beother surgically related intestinal disease such as carcinoma ,diverticulitis and Crohn s disease because ameboma canmimic colorectal carcinoma especially in the REPORTA 50 year-old, previously healthy male teacher presentedwith acute, dull aching, lower abdominal pain over the rightiliac fossa for two days.
4 There was associated fever with chillsand rigor. He experienced vomiting of two days duration,which was three episodes per day and mainly consisted ofclear fluids with food particles. He also experienced a fewepisodes of diarrhea prior to admission. He denied loss ofweight or bleeding per rectum and there was no familyhistory of colorectal cancer. There was also no history admission, he was febrile, lethargic and in pain. He hadtachycardia with normal blood pressure. Physicalexamination revealed a tense, guarded abdomen withrebound tenderness over the right iliac data showed leukocytosis with normal renal andliver functions. His serum carcinoembrionic antigen (CEA)level was normal at The serology (ELISA IgG)testing for amebiasis was negative, but the serology was sentonly after the histopathological examination.
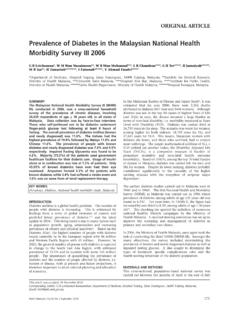
5 Stool for ovaand cysts were negative. The blood culture showed no underwent emergency operation on admission withsuspicion of a perforated appendix. However, the operationwas extended intra-operatively to a laparotomy with righthemicolectomy with primary end to end anastomosis forappendicular abscess and a suspected tumour over the were pus and multiple enlarged lymph nodes foundaround the ileocolic junction examination of the resected bowelrevealed acute inflammatory exudates and transmuralneutrophilic infiltrates within the terminal ileum andappendix. There were collections of pus cells with numeroustrophozoites resembling the macrophages ingesting red bloodcells; the features which were consistent with amoebic abscess (Figure 2).
6 Following resection of the ameboma, he received intravenouscefoperazone for a week and metronidazole for total of 2weeks duration. Subsequently, he made an uneventful post-operative recovery. To date, he has remained well andasymptomatic for 6 months following the surgery and theantibiotic therapy. This patient didn t receive anyintraluminal agents due to unavailability of the colonic amoebic abscess mimicking colonic carcinomaTan Li Peng, MRCP1, Kan Foong Kee, MRCP2, Yvonne Ai Lian Lim, PhD31 Department of Medicine, Hospital Pakar Sultanah Fatimah, Muar, Johor, 2 Department of Medicine, Hospital Sultanah Aminah,Johor Bahru, Johor, 3 Department of Parasitology, Faculty of Medicine, University of Malaya, Kuala LumpurCASE REPORTThis article was accepted: 2 August 2018 Corresponding Author: Li Peng TanEmail: colonic amoebic abscess mimicking colonic carcinomaMed J Malaysia Vol 73 No 5 October 2018335 DISCUSSIONC ases of ameboma mimicking intra-abdominal tumor orcarcinoma of colon had been reported before in countries likeJapan, Taiwan and India.
7 In previously reported cases, thepatients either presented with chronic diarrhea, abdominalpain, abdominal mass or even with complications likeperforative peritonitis. Some managed to have colonoscopyand biopsy done to diagnosed ameboma and henceappropriate treatment was ,2,3,4 Herein, we described a gentleman with amoebic abscess ofappendix and ileocaecal junction. The diagnosis of amebiasisin this case was challenging due to the presentation of anacute abdomen instead of chronic diarrhea. Furthermore,patient also didn t have other risk factors for amebiasis suchas poor sanitations or immunocompromised , it should be considered as one of the differentialdiagnosis in an amebiasis endemic is usually solitary and its size can be as large as15cm in diameter. It is more common among male and thoseaged between 20 to 60 years.
8 In terms of location, amebomadevelops most commonly in the caecum, followed by in theappendix then in the rectosigmoid region. Hepatic flexure,transverse colon and the splenic flexure have also beenreported as sites of diagnosis of amebiasis is made by demonstrating thepresence of cysts or occasionally trophozoites in stool, byimmunologic techniques or detection of the nucleic acid ofthe protozoan by PCR. Unfortunately, there are nopathognomic radiographic or endoscopic features which cansuggest of a possible invasive ameboma , strong clinical suspicion coupled with appropriateserology and tissue histopathologic confirmation is the key There is no established standard treatment strategy foramebic intra-abdominal tumour till date.
9 The managementcan be combination of both surgical resections with a courseof metronidazole. Following therapy for invasive amebiasis ,treatment with luminal agent to eliminate intraluminal cystsis warranted, even if stool microscopy is infection can be treated with one of thefollowing regimens: paromomycin (25 to 30 mg/kg per dayorally in three divided doses for 7 days), diiodohydroxyquin(650 mg orally TDS for 20 days) or diloxanide furoate (500mg orally TDS for 10 days).5 CONCLUSIONIt is difficult to differentiate ameboma with coloniccarcinoma from the equivocal clinical symptoms. Hence, thiscase was discussed in an attempt to highlight the possibilityof an ameboma mimicking colonic carcinoma , particularlyin an endemic region. Ameboma should be considered as oneof the differential diagnoses of masses located in the rightcolon (caecum and ascending colon), whereby the diagnosisrequires an early colonoscopy, histopathologic studies andblood/stool tests to check for the presence of intestinalamebiasis.
10 These measures will ensure early diagnosis andsubsequently to an appropriate authors would like to thank the Director General ofHealth Malaysia for his permission to publish this article. Wewould also like to express our deepest gratitude to DrNoorafidah Md Din, Pathologist of Hospital Pakar SultanahFatimah Muar for the HPE Wang SY, Shih SCh, Wang TE, Chang WH, Wang HY, Lin SC. Amebomamimicing submucosal tumor of the colon in an elderly. Int J Gerontology2011; 5: Ramachandran BS, Thomas B, Baby S, Thomas R. Multicentric amebomaof the colon mimicking Crohn s disease. J Dig Endosc 2015; 6: Sim ek H, Els rer R, S kmens er C, Balaban HY, Tatar G. Amebomamimicking carcinoma of the caecum: case report. Gastrointest Endosc2004; 59(3): Hardin RE, Ferzli GS, Zenilman ME, Gadangi PK, Bowne WB.